 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
1.1.2.1 Atopic dermatitis
ICD-11
EA80
Synonyms
Atopic eczema, endogenous eczema, neurodermatitis.
Epidemiology
Highly prevalent in infants and children (10-20%) and adults (2-8%).
Definition
Dermatitis in patients with atopic diathesis with a chronic-recurrent course, characterized by classical findings of dry skin, pruritus and textural change.
Read more
Atopic dermatitis is a chronic-recurrent eczema typically occurring in patients with atopic diathesis, characterized by classical findings of dry skin, pruritus, acute exudative flares, and scaly and thickened skin appearance in chronic phases.
Aetiology & Pathogenesis
- Genetically determined or acquired epidermal barrier defects (in some parts of the population mutation in profilaggrin gene and other structural epidermal proteins, alterations in the desquamation process), xerosis
- Genetically determined immune reaction pattern (excessive IgE production possible, disturbance in helper T-cell balance with Th2 favoured over Th1).
- Common triggers: environmental factors (humidity, water hardness, pollution), house dust mites, psychological stimuli.
Read more
Genetically determined or acquired epidermal barrier defects (structural and functional skin barrier impairment), in some parts of the population. Major role of loss-of-function mutations in profilaggrin gene and other structural epidermal proteins (e.g., hornerin, claudin and alterations in the desquamation process (e.g., stratum corneum proteases). These cause skin xerosis and higher skin permeability to exogenous irritants.
Genetically determined immune reaction pattern with excessive IgE production in most patients, due to disturbance in helper T-cell balance with Th2 immunity favoured. Th2 cytokines such as IL-4, IL-13 and IL-31 key mediators of pruritus and inflammation.
Common triggers: environmental factors (humidity, water hardness, pollution), house dust mites, psychological stimuli.
Signs & Symptoms
Eczema appearance with erythema and vesiculation in the acute phase and erythema, scaling and lichenification in the chronic phases. Another clinical feature is prurigo. Pruritus always present; it can be devastating and interfere with sleeping and work productivity.
Additional signs:
Dry skin (xerosis).
An atopy score (SCORAD, EASI, POEM) can be used to quantify diagnosis.
Read more
Eczema appearance with erythema and vesiculation in the acute phase and erythema, scaling and lichenification in the chronic phases. Skin may become thickened sometimes covered with scratch marks and even scars. Another clinical feature is prurigo. Pruritus is always present; it can be devastating and usually interfere with sleeping and work productivity, significantly affecting the quality of life. The patients are prone to develop secondary skin infections, bacterial or viral. Dry skin always present. Other clinical features include: nummular eczema and excoriated nodules (prurigo). Therefore, the clinical picture may be heterogenous (different phenotypes of atopic dermatitis). Several atopy scores (e.g., SCORAD, EASI, POEMS) have been developed to quantify disease severity
Localisation
- Localisation may be age dependent
- Face and neck
- Flexures (antecubital, popliteal, flexor aspect of wrist)
- Hands
- All parts of the body can be affected, even extending to erythroderma.
Classification
Intrinsic and extrinsic atopic dermatitis. Extrinsic: also defined allergic type, characterized by high total serum IgE levels and the presence of IgE to allergens; associated with asthma and/or rhino-conjunctivitis. Intrinsic: non-allergic, normal total serum IgE levels and the absence of specific IgE.
Read more
Intrinsic and extrinsic atopic dermatitis.
Extrinsic form, also defined as allergic type, accounts approximately for 80% of cases, characterized by high total serum IgE levels and the presence of specific IgE directed against the wide spectrum of environmental allergens; associated with asthma and/ or rhino-conjunctivitis.
Intrinsic form, also defined as non-allergic, approximately 20%, normal total serum IgE levels and no serum specific IgE to be detected.
Laboratory & other workups
Total serum IgE >100 kU/l, sometimes blood eosinophilia, often multiple positive skin prick tests, consider patch testing against airborne allergens after tape stripping of stratum corneum (atopic patch test).
Dermatopathology
Acute: spongiosis, perivascular lymphohistiocytic infiltrates in upper dermis. Chronic: parakeratosis, acanthosis, perivascular lymphohistiocytic infiltrates in upper dermis.
Read more
In the acute phase, the histology is characterized by epidermal spongiosis, perivascular lymphohistiocytic infiltrates and some eosinophilis in upper dermis. In the chronic, parakeratosis, mild spongiosis, acanthosis, and superficial perivascular lymphohistiocytic infiltrate.
Course
Chronic-relapsing course. Cradle cap after 3 months of age, weeping dermatitis in childhood, dry, itchy skin in adolescents and adults.
Read more
The course is chronic-relapsing. Cradle cap after 3 months of age, weeping dermatitis in childhood, dry, itchy skin in adolescents and adults. Atopic dermatitis has been associated with an increasing number of comorbidities, typically sharing some common pathological mechanism. In addition, there are cardiovascular, autoimmunological, neurological, psychological and other comorbidities which should be monitored in atopic dermatitis patients. The atopic march represents the natural progression of atopic diseases, is given by the deregulated epidermal barrier that facilitates allergic sensitization and starting with atopic dermatitis and followed by other atopic conditions, such as asthma, rhino-conjunctivitis. Many children outgrow the disease at school age or puberty. Early onset and severe cases persist into adulthood. About one third of adult cases is new onset disease (late and very late onset atopic dermatitis).
Complications
Tendency to superinfection by bacteria (Staph. aureus: impetiginization) and viruses (eczema herpeticum/molluscum contagiosum).
Read more
Tendency to superinfection by bacteria (Staphylococcus aureus: impetiginization) and viruses (eczema herpeticum/ molluscum contagiosum). Eczema herpeticum may be complicated by visceral involvement (pneumonia).
Diagnosis
Typical personal and family history, characteristic clinical picture, relevant laboratory tests, often coexisting atopic disorders (allergic rhinitis, conjunctivitis, asthma or type 1 food allergies).
Differential Diagnosis
Seborrhoeic dermatitis, psoriasis, allergic contact dermatitis, tinea, scabies, early patch stage mycosis fungoides.
Read more
Differential diagnosis includes seborrhoeic dermatitis, psoriasis, allergic contact dermatitis, nummular eczema, tinea, scabies, early patch stage mycosis fungoides.
Prevention & Therapy
1. General measures:
- Counselling regarding skin care, avoidance of aggravating factors. Patient handouts and educational material or links are valuable.
- Moisturising, often with emollients containing urea.
- Gentle cleansing (use of soap substitutes).
2. Mild forms:
- Topical corticosteroids, perhaps combination products also containing antimicrobial agents (short-term to avoid bacterial resistance).
- Topical immune modulators (tacrolimus, pimecrolimus, crisaborole).
3. Severe forms:
- Ciclosporin or other immunosuppressants (methotrexate, azathioprine, mycophenolate mofetil).
- Short-term systemic corticosteroids.
- Biological therapy: Dupilumab, a human monoclonal antibody directed against IL-4/IL-13 receptor-α.
- Several new treatments under development.
Read more
1. General measures:
Counselling regarding skin care, avoidance of triggering factors. Patient handouts and edu cational material or links are valuable.
Moisturising, often with emollients containing urea, bacterial lysates (eg. Vitroscilla filliformis) and other factors.
Gentle cleansing (use of soap substitutes).
Elimination of triggering environmental factors
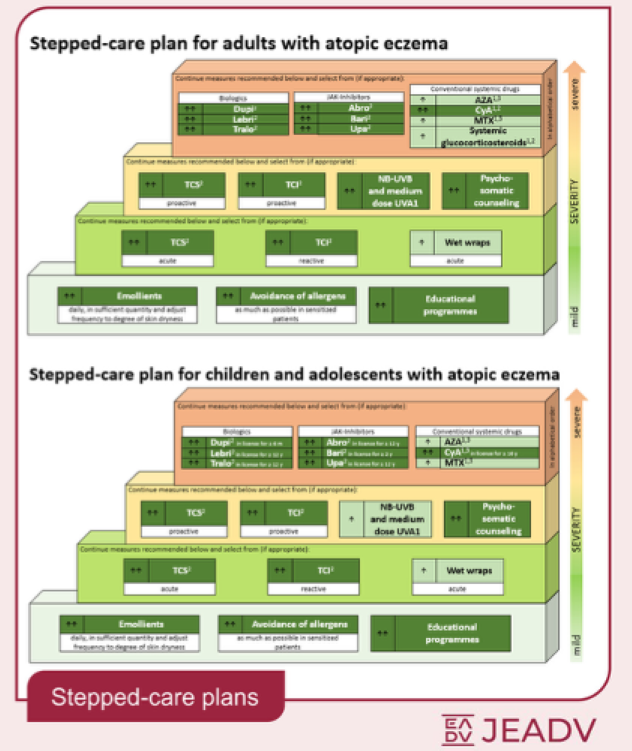
Graphic 2 illustrates a stepped-care approach for adults and children with atopic dermatitis, according to the 2025 European Guideline (EuroGuiDerm) on atopic eczema.
2. Mild forms:
Topical corticosteroids, including combined products containing additional antimicrobial agents (short-term to avoid bacterial resistance).
Topical immune modulators (tacrolimus, pimecrolimus, crisaborole).
3. Severe forms:
Cyclosporine A or other systemic immunosuppressants (methotrexate, azathioprine, mycophenolate mofetil).
Short-term systemic corticosteroids.
Biological therapy: Dupilumab is a human monoclonal antibody directed against IL-4/IL-13 receptor-α chain and thus block both IL-13 and IL-4. Tralokinumab and lebrikizumab are monoclonal antibodies that block IL-13. They are not generally immunosuppressive and do not require laboratory screening and monitoring. Dupilumab licensed from age of 6 months; lebrikizumab and and tralokinumab from age 12.
Janus kinase (JAK) inhibitors: Abrocitinib and upadacitinib, JAK1 selective inhibitors; baricitinib, a JAK1 and JAK2 inhibitor. Abrocitinib and upadacitinib are a bit more rapidly efficacious than dupilumab but have some contraindications and require laboratory screening and monitoring. Upadacitinib licensed from age 12. Oral JAK inhibitors have a black box warning on increased risk of developing serious infections, major cardiovascular events, venous thromboembolism and malignancy. Accumulating real world studies are reassuring about safety concern.
Other new treatments under development.
4. Prevention:
Intensive and regular use of skin emollients and ointments, in every age. Prevention is important to minimize the occurrence of asthma and rhino-conjunctivitis (atopic march). Proactive use of topical drugs significantly reduces frequency of relapses.
Differential Diagnosis
Further images / DOIA
Review Articles
References
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment