 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
1.1.2.2 Allergic contact dermatitis
ICD-11
EK00
Synonyms
Allergic contact eczema, contact dermatitis.
Epidemiology
An estimated 15–20% of the general population suffers from contact allergy
Definition
Allergic contact dermatitis is a common type of dermatitis caused by delayed hypersensitivity reaction (type IV) to exogenous (contact-) allergens (haptens) in contact with the skin.
Aetiology & Pathogenesis
Allergic contact dermatitis is mediated by allergen-specific sensitized T cells and is a form of type IV reaction, according to Gell and Coombs. Immunological sensitization time is at least 5-10 days; clinical symptoms may first develop after months to years. The dermatitis appears in sensitised individuals after a latency period of 8-24 hours, occasionally longer. Individual allergens have varying degrees of allergic potential. Most frequent contact allergens are metals, rubber ingredients, preservatives and occupational substances.
Read more
Allergic contact dermatitis is mediated by allergen-specific sensitized T-cells and is a form of type IV reaction, according to Gell and Coombs. Immunological sensitization time is at least 5-10 days; clinical symptoms may first develop after months to years. The dermatitis appears in sensitised individuals after a latency period of 8-24 hours, occasionally longer. Individual allergens have varying degrees of allergic potential. Most frequent contact allergens are:
Metals (e.g. nickel in ear jewelry, jeans buttons, coins)
Fragrances (in cosmetics, hygiene products, industrial products),
Natural substances (such as resin, balsam of Peru, compositae (aster, daisy, sunflower family),
Rubber ingredients (rubber additives such as thiurams, carbamates),
Preservatives (such as isothiazolinone, methyl-3-bromo-butyronitril, formaldehyde),
Occupational substances (such as epoxies, chrome salts (cement and leather), p-phenylenediamine).
Aerogen / airborne delivered contact allergens
Signs & Symptoms
The reaction starts at the site of allergen exposure as an acute papulo-vesicular eruption which soon becomes eroded and forms an exudate. It is accompanied by intense pruritus. The lesions present with irregular border, spreading outside area of contact. Later, scaling and crusting can occur. In chronic forms, lichenification and fissuring dominate. Sometimes, allergic contact dermatitis may present as a chronic disease without an acute clinical phase.
Localisation
The localisation depends on the type of exposure. Extensive (haematogenous) contact dermatitis may by caused by systemic exposure (ingestion, inhalation) of contact allergens. The affected site is a clue to the possible culprit allergen. Face: cosmetics, airborne allergens (paint vapours or pollens). Ears: jewellery, glasses, hearing aids. Lips: cosmetics, herpes simplex medications. Forehead/neck: shampoos, hair dyes. Neck/fingers/wrist: jewellery. Hands: occupational and recreational contact allergens. Axillae: deodorants. Feet: shoes, antifungals. Mouth: dentures, other dental products. Lower leg: elastic stockings, medications for leg ulcers.
Laboratory & other workups
The allergen causing contact dermatitis may be determined by patch testing. Several series of patch tests can be used: standard series of most frequent allergens, special series for peculiar occupational diseases, own substances brought by the patient. ROAT (repeated open application test) may be useful for low allergenic substances.
Read more
The allergen causing contact dermatitis may be determined by patch testing. Several series of patch tests may be used: standard series of most frequent allergens, special series for selected occupational diseases, emollients or any other substances suspected to be a causative factor (delivered by the patients) may be also tested. ROAT (repeated open application test) may be useful for low allergenic substances and selected topical medications.
Dermatopathology
Cutaneous histology of the lesions shows parakeratosis, spongiosis, acanthosis, and an inflammatory lymphohistiocytic infiltrate with exocytosis of lymphocytes into epidermis.
Course
The clinical features usually subside after 1-2 weeks of allergen avoidance; contact sensitivity usually persists indefinitely.
Read more
The clinical features usually subside after 1-2 weeks of allergen avoidance; contact sensitivity usually persists lifelong via memory T-cells.
Complications
Allergic contact dermatitis can be complicated by impetiginization, the disease can become chronic (even after allergen avoidance). The lesions can disseminate and cause erythroderma.
Diagnosis
It is mandatory to seek the causative allergen by performing detective work (detailed history - work, hobbies, habits), and patch testing oriented by the history.
Differential Diagnosis
Allergic contact dermatitis must be differentiated from other inflammatory diseases such as psoriasis and dermatophyte infection in case of foot and hand involvement. It must also be differentiated from therapy-resistant localized dermatitis: Bowen’s disease, Paget’s disease of the nippleand lupus vulgaris. Reaction to latex can cause an IgE-mediated immediate type allergy in addition to a type IV allergic reaction to rubber accelerators.
Read more
Allergic contact dermatitis must be differentiated from other inflammatory diseases such as psoriasis and dermatophyte infection in case of foot and hand involvement. It must also be differentiated from therapy-resistant localized dermatitis: Bowen’s disease, Paget’s disease of the nipple, lupus vulgaris. Reaction to Latex can cause an IgE-mediated immediate type allergy in addition to a type IV allergic reaction. A subtype is eczema in psoriatic in which psoriasis of palms and soles may provoked or maintained by contact allergens.
New allergens are constantly being registered as possible causative haptens in allergic contact dermatitis (update of the patch tests series, profession/occupation-related haptens containing series, etc.).
Prevention & Therapy
It is very important to avoid contact with the causative allergens, and also with concomitant irritants (e.g. by using soap substitutes). Topical therapy consists of wet dressings or baths, and mainly corticosteroids in the appropriate vehicle (ointment, cream, lotion) chosen according to the nature of skin lesions. Phototherapy may be indicated in some cases. Alitretinoin (retinoid) can be used in severe refractory hand dermatitis.
Read more
It is very important to avoid contact with the causative allergens, and also with additional irritating factors (for example, using soap substitutes). Topical therapy consists of wet dressings or baths, and mainly corticosteroids as well as calcineurin inhibitors. An appropriate vehicle (ointment, cream, lotion) should be selected according to the morphological characteristics of skin lesions. Phototherapy may be indicated in some cases. Oral alitretinoin (retinoid) may be effective in severe refractory hand dermatitis.
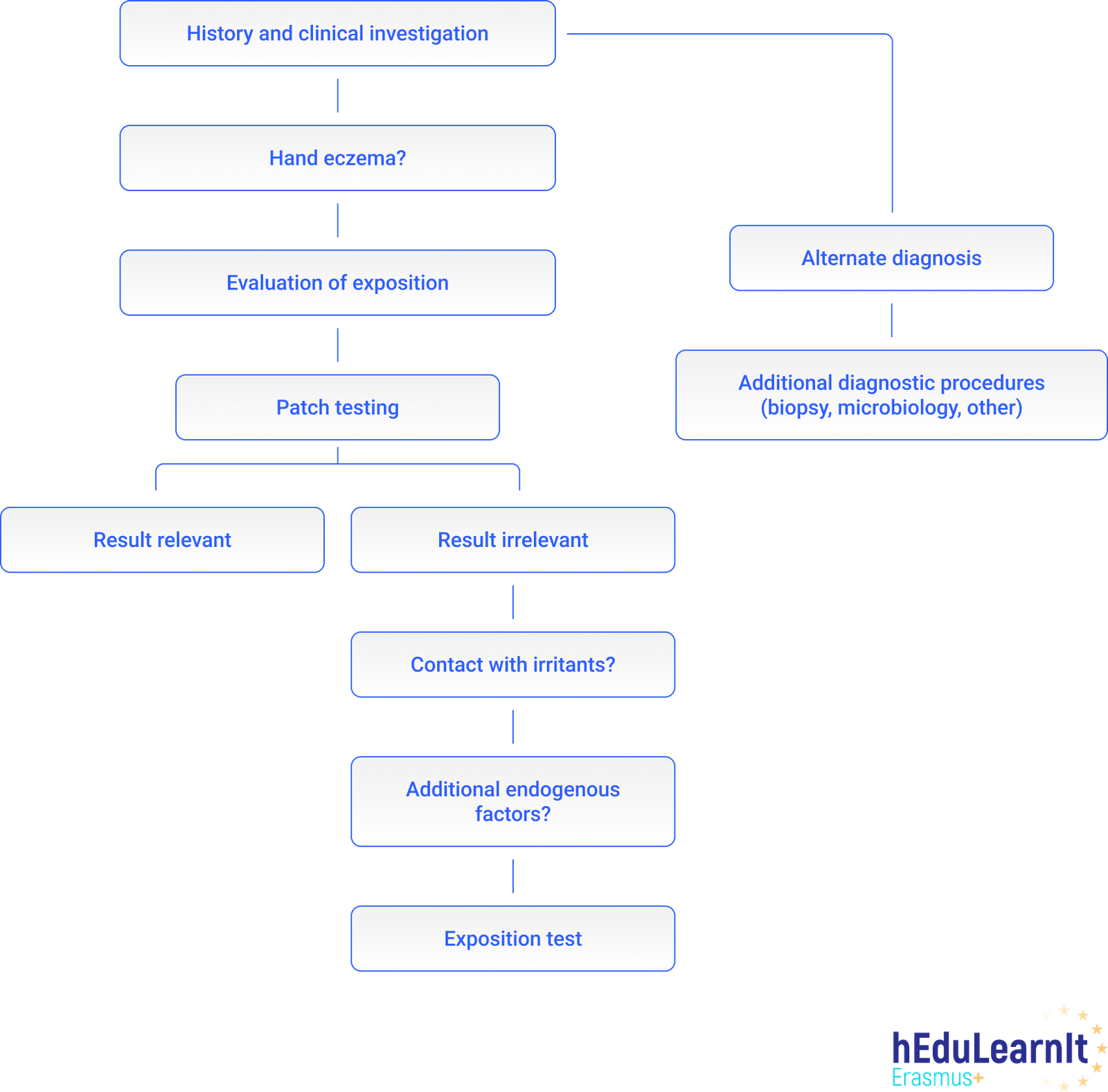
Diagnostic algorithm
Differential Diagnosis
Podcasts
Tests
- Which are (or used to be) the sources of exposure for chromate?
- Statement 1: The Location of an allergic contact eczema may indicate the responsible allergen
- Which efflorescence is not typical for acute allergic contact dermatitis?
- Which diseases belong to the differential diagnosis of allergic contact dermatitis?
- Allergic contact dermatitis can appear at the following sites:
- Which of the statements apply to allergic contact dermatitis?
- Statement 1 If a Type IV allergy is identified, the antigen must be completely avoided
- Statement 1 Acute allergic contact dermatitis may require the use of systemic corticosteroids
- Which of these is the cause of allergic contact dermatitis?
- Which medication is not appropriate for acute allergic contact dermatitis?
- Which statements about allergic contact dermatitis are true?
- Which type of lesion or finding is not typical for allergic contact dermatitis?
Further images / DOIA
Review Articles
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment