 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
1.4.1 Sarcoidosis
ICD-11
4B20
Synonyms
Boeck disease, Besnier-Boeck-Schaumann disease, benign lymphogranulomatosis.
Epidemiology
Rare disease. Skin involvement in 20-35% of cases; in 11% skin as first manifestation. The estimated prevalence in Europe is around 10/100,000 inhabitants, and is significantly higher in northern countries.
Read more
Rare disease. Skin involvement in 20-35% of cases; in 11% skin as first manifestation.
The estimated prevalence in Europe is around 10/100,000 inhabitants, and is significantly higher in northern countries. A bimodal age distribution between the ages of 25 and 35 years and between 45 and 65 years was reported.
Definition
Systemic granulomatous disease with skin involvement.
Aetiology & Pathogenesis
Unclear, found worldwide, female > male. It occurs most commonly in young and middle-aged individuals of both genders and all races. Afro-Caribbeans and African-Americans more commonly involved.
Read more
Still unclear, found worldwide, female > male. It occurs most commonly in young and middle-aged individuals of both genders and all races with Afro-Caribbeans and African-Americans more commonly involved. It is a primary Th1 cell driven disease, however, multiple other T-cell types including Th17, Th17.1 cells, and T regulatory cells are involved. In building up granulomas, maintaining or resolving those a pattern of different cytokines, i.e., transforming growth factor-ß (TGF-ß), IL-13 and IL-10 are involved. Several drugs as trigger factor in particular during or after oncologic immunotherapy with CTLA-4 and PD-1/PD-L1 inhibitors25 and during tumor necrosis factor (TNF) inhibition as well as with recombinant type 1 interferon (α and β) therapy have been reported.
Signs & Symptoms
Many possible skin findings: brown-violaceous dermal papules, plaques, nodules. Often associated with erythema nodosum. Systemic disease can involve lymph nodes (90%, mostly intrathoracic), lungs (90%), eyes (30%), kidneys, bones, neural system, liver and GI tract.
Localisation
All skin areas can be involved.
Classification
Special forms:
- Löfgren's syndrome (acute onset of fever, bilateral hilar lymphadenopathy and erythema nodosum)
- Lupus pernio (centrofacial skin involvement)
- Scar and tattoo sarcoidosis
Read more
Two standardized outcome instruments exist—the Sarcoidosis Activity and Severity Index (SASI) and the Cutaneous Sarcoidosis Activity and Morphology Instrument (CSAMI).
Special forms:
Löfgren’s syndrome (acute onset of fever, bilateral hilar lymphadenopathy and erythema nodosum, 5%).
Lupus pernio (centrofacial skin involvement).
Scar and tattoo sarcoidosis.
Rare forms, e.g. Heerfordt’s syndrome (uveitis, parotid gland swelling, chronic fever, occasionally palsy of the facial nerve, 1%).
Laboratory & other workups
- Angiotensin converting enzyme (ACE; indicating cumulative involvement) and interleukin 2 receptor (IL2R; indicating disease activity) in serum sometimes elevated
- Hypercalcemia
- Lymphopenia
- ESR elevated
- Impaired delayed (type IV) hypersensitivity
- Tuberculin skin test (negative)
- Chest x-ray (may show bilateral hilar lymphadenopathy or interstitial changes)
Read more
Angiotensin converting enzyme (ACE; indicating cumulative involvement) and interleukin 2 receptor (IL2R (CD25); indicating disease activity) in serum sometimes elevated
Hypercalcaemia
Lymphopaenia
ESR elevated
Impaired delayed (type IV) hypersensitivity
Tuberculin skin test (negative) / Quantiferon test
Chest x-ray (may show bilateral hilar lymphadenopathy or interstitial changes)
Dermatopathology
Epithelioid cell granulomas without caseation, few CD4+ T lymphocytes (naked granulomas).
Course
Chronic, spontaneous remission (25%).
Complications
Restrictive lung disease, immune suppression (lymphopenia), osteoporosis (in corticosteroid-treated patients; calcium supplementation contraindicated). Cutaneous calcification (calcinosis cutis).
Diagnosis
Clinical features, histology, laboratory findings.
Differential Diagnosis
Tuberculosis, leprosy, granuloma annulare, necrobiosis lipoidica, lymphoma, leishmaniasis, amyloidosis, rosacea (lupus pernio).
Read more
Tuberculosis, leprosy, granuloma annulare, necrobiosis lipoidica, lymphoma and pseudolymphoma, leishmaniasis, syphilis, rosacea (lupus pernio).
Prevention & Therapy
Prevention of occupational and individual chronic small particle inhalation:
- Skin involvement: Corticosteroids (topical, intralesional, systemic; first line), methotrexate (second line), chloroquine/hydroxychloroquine, PUVA
- Systemic involvement: Corticosteroids (systemic; first line), methotrexate (second line), azathioprine, (leflunomide, mycophenolate mofetil, cyclophosphamide, TNF antagonists. Biologics may induce sarcoidosis.
Read more
Prevention of occupational and individual chronic small particle inhalation
Skin involvement: Corticosteroids (topical, intralesional, systemic; first line), methotrexate (second line), chloroquine/hydroxychloroquine, (isotretinoin, allopurinol, thalidomide), PUVA
Systemic involvement: Corticosteroids (systemic; first line), methotrexate (second line), azathioprine, (leflunomide, mycophenolate mofetil, cyclophosphamide), TNF antangonists. JAK inhibitors are one of the most important potential therapeutic agents for sarcoidosis currently under investigation. Some biologics may induce sarcoidosis.
Special
Sarcoidosis is probably one of the systemic diseases in which the environment has the greatest influence on the disease development (people with specific occupations).
Diagnostic algorithm
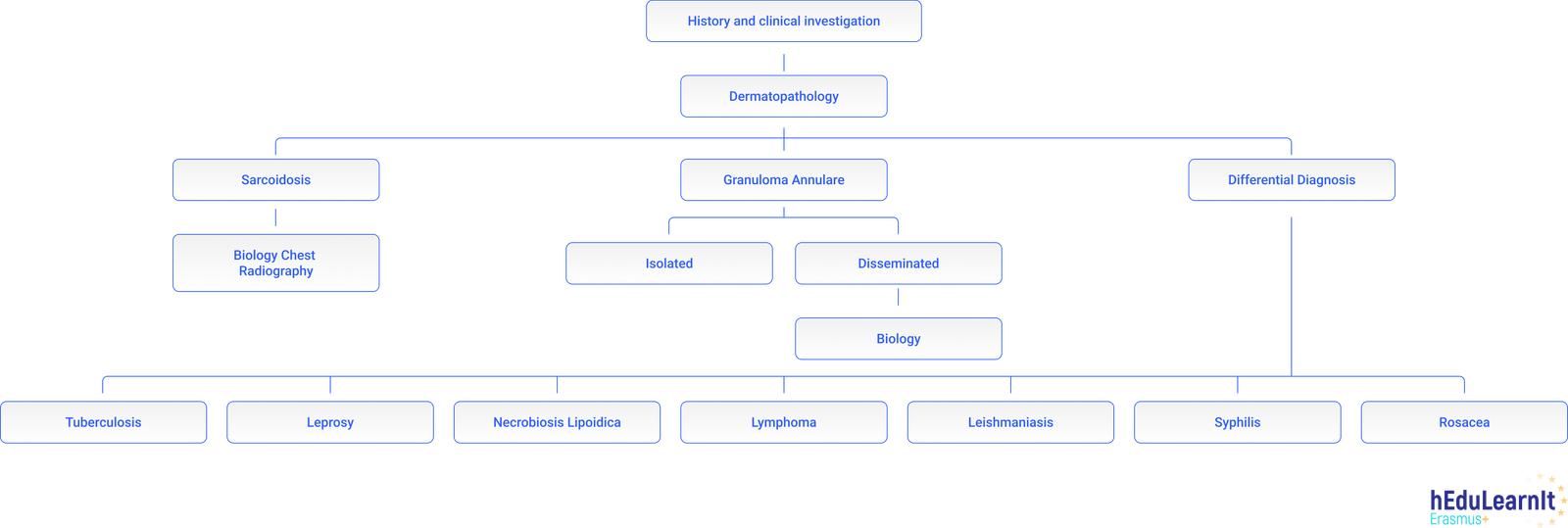
Differential Diagnosis
Podcasts
Tests
- This patient with AIDS Stage C3 has developed red-brown facial papules over the past few weeks. A skin biopsy shows dermal granulomas. What should you consider in your differential diagnosis?
- Statement 1 Sarcoidosis not only involves the skin but also the lungs, eyes, salivary glands, kidneys, bones, tonsils and nervous system.
- Sarcoidosis with cutaneous, pulmonary and renal involvement in a 25-year-old woman from the Antilles. The chest x-ray shows parenchymal diseases with micronodular lesions. What treatment do you suggest?
- 55-year-old woman presents with facial dermatosis for several months. Differential diagnostic possibilities include
- True or false?
- This young lady has increasing dyspnea and disseminated brown papules. The biopsy is compatible with sarcoidosis, What other tests are indicated?
- This young lady has numerous red-brown papules which have a yellow color under diascopy. The biopsy shows epithelioid granulomas without central necrosis. The likely diagnosis is?
- Young lady from Finland with fever (39 °C), arthralgias, and painful lesions on legs. The chest x-ray shows perihilar infiltrates with mediastinal lymphadenopathy. What is the diagnosis?
Further images / DOIA
Review Articles
- M.C. Iannuzzi, B.A. Rybicki, A.S. Teirstein: Sarcoidosis (2017)
- A. Haimovic, M. Sanchez, M.A. Judson, S. Prystowsky: Sarcoidosis: A comprehensive review and update for the dermatologist: Part I. Cutaneous disease (2012)
- A. Haimovic, M. Sanchez, M.A. Judson, S. Prystowsky: Sarcoidosis: A comprehensive review and update for the dermatologist: Part II. Extracutaneous disease (2012)
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment