 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
3.1.1 Melanocytic Nevus
ICD-11
2F20.Z
Synonyms
Mole, sometimes just called “nevus”.
Epidemiology
Melanocytic naevi are very common (even ubiquitous, even in African populations) and may be present at birth. The number of melanocytic naevi increases with age until the age of around 50 years but there may be involution over time as well. A new melanocytic lesion appearing after the age of 30 years should raise clinical suspicion for malignant melanoma.
Definition
Acquired benign neoplasms of melanocytic lineage are termed melanocytic nevi (the plural of nevus). They are collections of melanocytes (naevus cells) in the epidermis, dermis or both.
Read more
Acquired benign neoplasms of melanocytic lineage are termed melanocytic nevi (plural of nevus). Melanocytic nevi are collections of melanocytes (nevus cells) in the epidermis (junctional nevus), dermis (dermal nevus) or both (compound nevus).
Aetiology & Pathogenesis
Acquired melanocytic nevi express a high diversity of clinical appearance and histomorphology, age of onset mostly during first two decades of life, anatomic site, and genetic alterations. Melanocytes arise from the neural crest and migrate to the skin during embryogenesis. Most melanocytic naevi appear during the first two decades of life. Increased exposure to UV light in childhood seems to be a promoting factor, particularly episodes of sunburn. Melanocytic nevi tend to disappear with aging.
Read more
Melanocytes are derived from the neural crest during embryogenesis. Two developmental pathways give rise to melanocyte progenitor cells. The dorsolateral pathway generates melanoblasts that travel through the mesoderm to colonize the epidermis, mucosa, and hair follicles. A second population of neural crest cells gives rise to bipotent precursors of Schwann cells and melanocytes that migrate ventromedially to reach the skin.
Acquired melanocytic nevi express a high diversity of clinical appearance and histomorphology. Age of onset mostly during first two decades of life. Common acquired nevi have the highest BRAF mutation frequency. Increased exposure to UV light in childhood seems to be a promoting factor. Melanocytic nevi tend to disappear with aging.
Signs & Symptoms
These skin-coloured or mostly pigmented macular, papular or nodular lesions are usually asymptomatic, but can occasionally be itchy or uncomfortable if irritated. They should be symmetrical, with a smooth outline, homogeneous, with a regular border, of small diameter (<6 mm) and stable over time. (see ABCDE rules/’ugly duck’ concept in the Melanoma chapter; for Atypical melanocytic nevus see chapter 9.7.).
Read more
Lesions present as mostly pigmented or less commonly skin-coloured macular, papular or nodular lesions. Atypical (by dermpathology dysplastic) nevi are often asymmetrical with a red-brown border and non-homogenous pigmentation. They fulfil the ABCD(E) rules, different melanoma types are a differential diagnosis and must be ruled out (see Melanoma and atypical nevi 9.7.).
Localisation
Melanocytic nevi may occur anywhere on the body, sometimes on the oral and genital mucosa or in the sclera or retina of the eye.
Read more
Melanocytic nevi may occur anywhere on the body, the scalp or plantar surfaces, interdigital folds, the umbilicus or sometimes on the oral and ano-genital mucosa.
Classification
Variants: junctional nevus, dermal nevus and combination of both compound nevus; blue nevus, combined nevus ( acquired plus blue nevus), Mongolian spot, congenital (hairy) nevus, halo naevus. Spindle- and epithelioid cell nevus.
Read more
There are several variants of melanocytic nevi which include: common acquired nevus, congenital nevus, blue nevus, Mongolian spot, congenital (hairy and non-hairy) nevus (including small, medium, large and giant), halo nevus, Spit/Reed nevus, Wiesner nevus, combined nevus and nevi associated with syndromes. A halo nevus is a mole surrounded by a white ring. These halo naevi are also called Sutton nevi. They are more common in children and young adults.
Laboratory & other workups
No laboratory tests are needed.
Dermatopathology
Proliferation of melanocytes, single or in nests, epidermal (junctional nevus), dermal (dermal nevus), or at both levels (compound nevus). Melanocytic naevi with histological signs of atypia are referred to as dysplastic naevi (see separate chapter 9.7 Atypical melanocytic nevus).
Read more
The histological examination shows increased melanocytic cells, single or in nests in the basal layer of the epidermis or dropping down in the dermis. This helps distinguish between epidermal proliferation of melanocytes (junctional nevus), dermal proliferation (dermal nevus), or proliferation at both levels (compound nevus). Often macrophages storing melanin pigment can be found. Melanocytic nevi with histological signs of atypia are referred to as dysplastic nevi.
Course
Progression towards atypical melanocytic nevi possible, for melanoma is exceptional (except in cases of giant congenital nevus, see chapter 3.1.6 Congenital Melanocytic Nevus), but patients with more than 100 nevi are at higher risk of developing a melanoma. Multiple enlarged acquired nevi have increased melanoma risk.
Complications
The number of melanocytic naevi (>50-100), along with skin type and history (severe sunburns in childhood) are the most important risk factors for melanoma. Irritated or excoriated naevi are sometimes mistaken for cancer.
Read more
ABCDE rules/’ugly duck’/’mole out of context’ concept may help distinguish benign from malignant lesions. The diagnosis is generally made on clinical features alone. Dermatoscopy (where images are magnified x10) is a useful tool to increase diagnostic accuracy. Histological examination is required if the lesion is clinically unusual to rule out melanoma.
Diagnosis
ABCDE rules/’ugly duck’/’mole out of context’ concept may help distinguish benign from malignant lesions. Clinical features, dermatoscopy (where images are magnified x10), histology.
Read more
ABCDE rules/’ugly duck’/’mole out of context’ concept may help distinguish benign from malignant lesions. The diagnosis is generally made on clinical features alone. Dermatoscopy (where images are magnified x10) is a useful tool to increase diagnostic accuracy. Histological examination is required if the lesion is clinically unusual to rule out melanoma.
Differential Diagnosis
Other pigmented, usually acquired skin lesions including seborrheic keratosis, pigmented basal cell carcinoma; less often dermatofibroma, haemangioma. Different subtypes of early melanomas.
Read more
The differential diagnosis includes other pigmented, usually acquired skin lesions such as
early melanoma,
pigmented seborrheic keratosis (melanoacanthoma),
pigmented basal cell carcinoma;
less often histiocytoma, haemangioma, fibroma.
Prevention & Therapy
Abstention, excision if there is esthetic discomfort, irritated nevi by trauma or localization or in case of atypical nevi or suspicious melanoma.
Excision if there is an irritated nevus by trauma or localization with constant irritation. Usually observation/ abstention (using the ABCDE rules to guide decision) if there is diagnostic doubt or functional problems. Digital images in the clinical record may be helpful to facilitate accurate long-term follow-up. Visible change in the digital record within three months of follow-up is an absolute indication for excision.
Read more
Observation (using the ABCDE rules to guide decision by the patient or clinician) is encouraged, but sometimes excision is required if there is diagnostic doubt or functional problems. Digital images in the clinical record may be helpful to facilitate accurate long-term follow-up. Visible change in the digital record within three months of follow-up is an absolute indication for excision. Abstention is preferred if there is no suspicion of atypical nevi. Excision may be performed if there is aesthetic discomfort, irritated nevi by trauma or localization or in case of a suspicious melanoma. Patients with giant congenital nevi or high numbers of dysplastic nevi must be regularly screened for melanoma.
Special
None.
Diagnostic algorithm
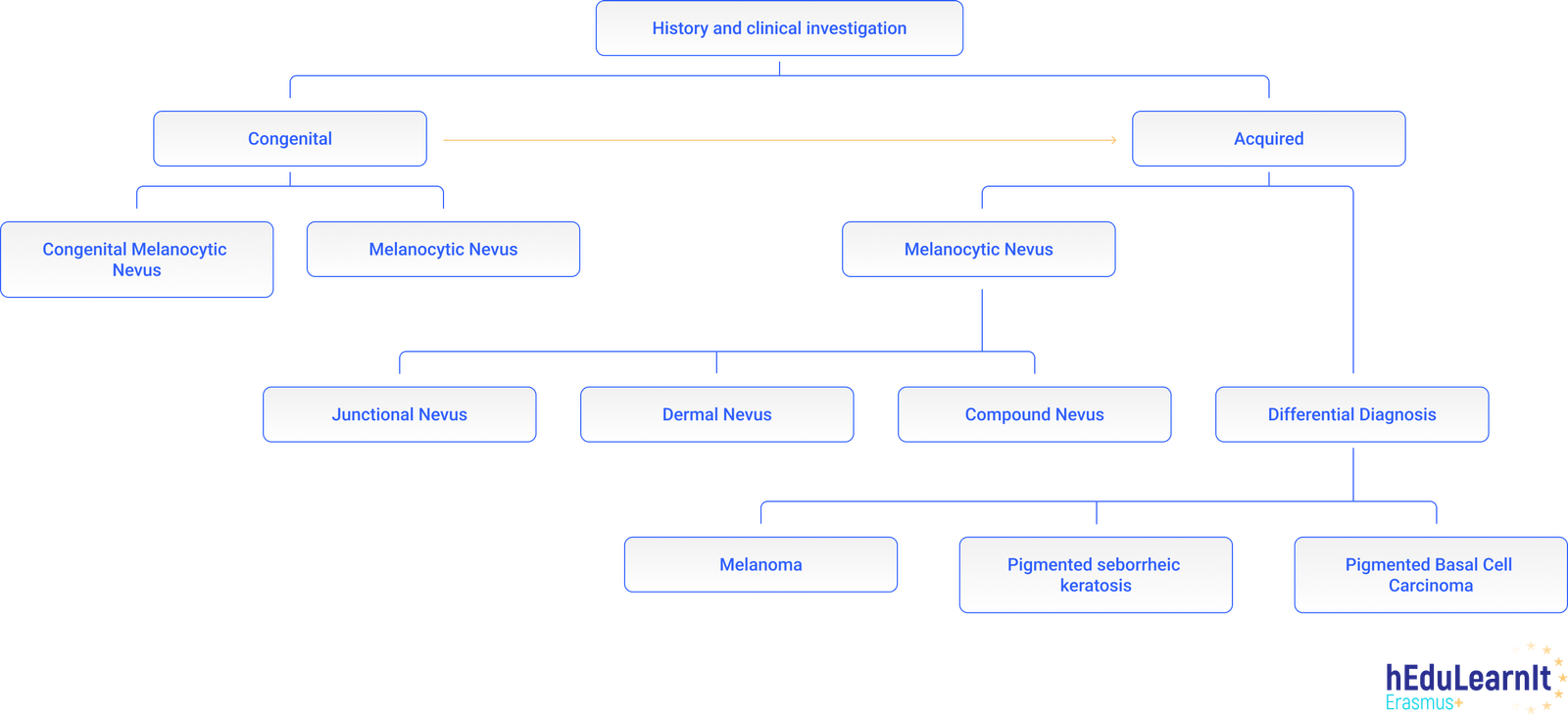
Differential Diagnosis
Cases
Podcasts
Tests
- Melanocytic nevi are always precursors of malignant melanomas
- Melanocytic nevi are always acquired
- Malignant melanoma is one of the most aggresive tumors existing
- A melanocytic nevus which is suspected of being a melanoma should be surgically removed
- A melanocytic nevus which is suspected of being a melanoma should not be removed with laser destruction
- Statement 1 If an melanocytic nevus is not completely excised, it should be re-excided with 1 cm safety margins
- Statement 1 Melanocytic nevi are always precursors of malignant melanomas
- Statement 1 Melanocytic nevi are always acquired
- Statement 1 Malignant melanoma is a very aggressive tumor
- Statement 1 A suspicious melanocytic nevus should be excised
- Statement 1 Melanocytic nevi are a heterogenous group of benign melanocytic lesions
- Statement 1 A melanocytic nevus which is suspected of being a melanoma should not be removed with laser destruction
- Statement 1 Regular UV light exposure is a good preventive measure to avoid developing new melanocytic nevi
Further images / DOIA
References
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment