 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
4.2.2 Androgenetic Alopecia
ICD-11
ED70.0
Synonyms
Male pattern hair loss; common balding; male-pattern baldness; hormone-related alopecia; pelade.
Read more
Male pattern hair loss; common balding; male-pattern balding; male-pattern baldness; hormone- induced alopecia.
Epidemiology
30-40% of women will have thinning hair by the age of 70 or older.
50-60% of men have a bald scalp by 70 years (but may start earlier, especially with a positive family history).
The condition is less commonly seen in men of East Asian ancestry.
Read more
30-40% of women will have thinning hair by the age of 70 or older. 50-60% of men have a bald scalp by 70 years. Early-onset AGA (<30 years of age) is most common in men of South Asian ancestry with a higher than average overall AGA prevalence of 58% during their fifties. AGA occurs with lower frequencies in men of Central European descent (50% in men in their fifties) and African descent. East Asian men are consistently reported as less affected than men of European ancestry throughout all decades of life.
Definition
Progressive androgen-dependent hair loss in typical locations associated with genetic predisposition and natural aging. In women, early aggressive disease or specific pattern (Hamilton-Norwood) of hair loss may indicate an endocrine disorder.
Read more
Androgenetic alopecia is a non-scarring, progressive, androgen-dependent form of hair loss/hair follicle rarefication. It shows progressive miniaturization of hair follicles and a reduction in the number of active follicles. It occurs in typical locations (different patterns for women and men) associated with a genetic predisposition and natural aging. In women, early aggressive disease or a Hamilton-Norwood pattern of hair loss may indicate an endocrine disorder.
Aetiology & Pathogenesis
Polygenic inheritance. Abnormalities of local follicular androgen metabolism, especially increased activity of 5α-reductase, lead to increased levels of dihydrotestosterone.
Read more
There is polygenic inheritance. Abnormalities of androgen metabolism, especially enhanced activity of 5α-reductase, lead to increased levels of dihydrotestosterone in target organ. However, several other enzymes (aromatase pattern) and hormones of the androgen metabolism pathway are associated. More than 380 genomic loci associated with AGA, including genes involved in androgen and WNT pathways have been detected.
Signs & Symptoms
Progressive and persistent asymptomatic hair loss in symmetrical pattern.
Read more
The hair loss in young male patients is progressive and persistent, but generally asymptomatic. Very occasionally scalp pain (known as trichodynia) can be a feature of the hair loss. The hairs are lost in a symmetrical pattern. Frontal, mid-scalp and occipital hair follicles in postpubescent men and in postmenopausal women are susceptible. In women and older men, usually normal levels of hair loss occur, however, hair regrowth is markedly diminished and hair shafts are thinner. In these cases “hair follicle rarefication” and not hair loss represents the term properly describing the disorder.
Localisation
Women - thinning of centro-parietal scalp, with widened parting but retained anterior hair line. The clinical pattern is variable and can be diffuse. Never complete hair loss on vertex.
Men - bi-temporal symmetrical regression, thinning of the vertex, later more complete loss leaving a residual parietal-occipital band.
Read more
Women show thinning of centro-parietal scalp, with a widened parting but retained anterior hair line. The clinical pattern is variable and can be diffuse. There is never complete hair loss on the vertex.
Men typically show bi-temporal symmetrical regression, thinning of the vertex, but later, more complete loss leaving a residual parietal-occipital band intact.
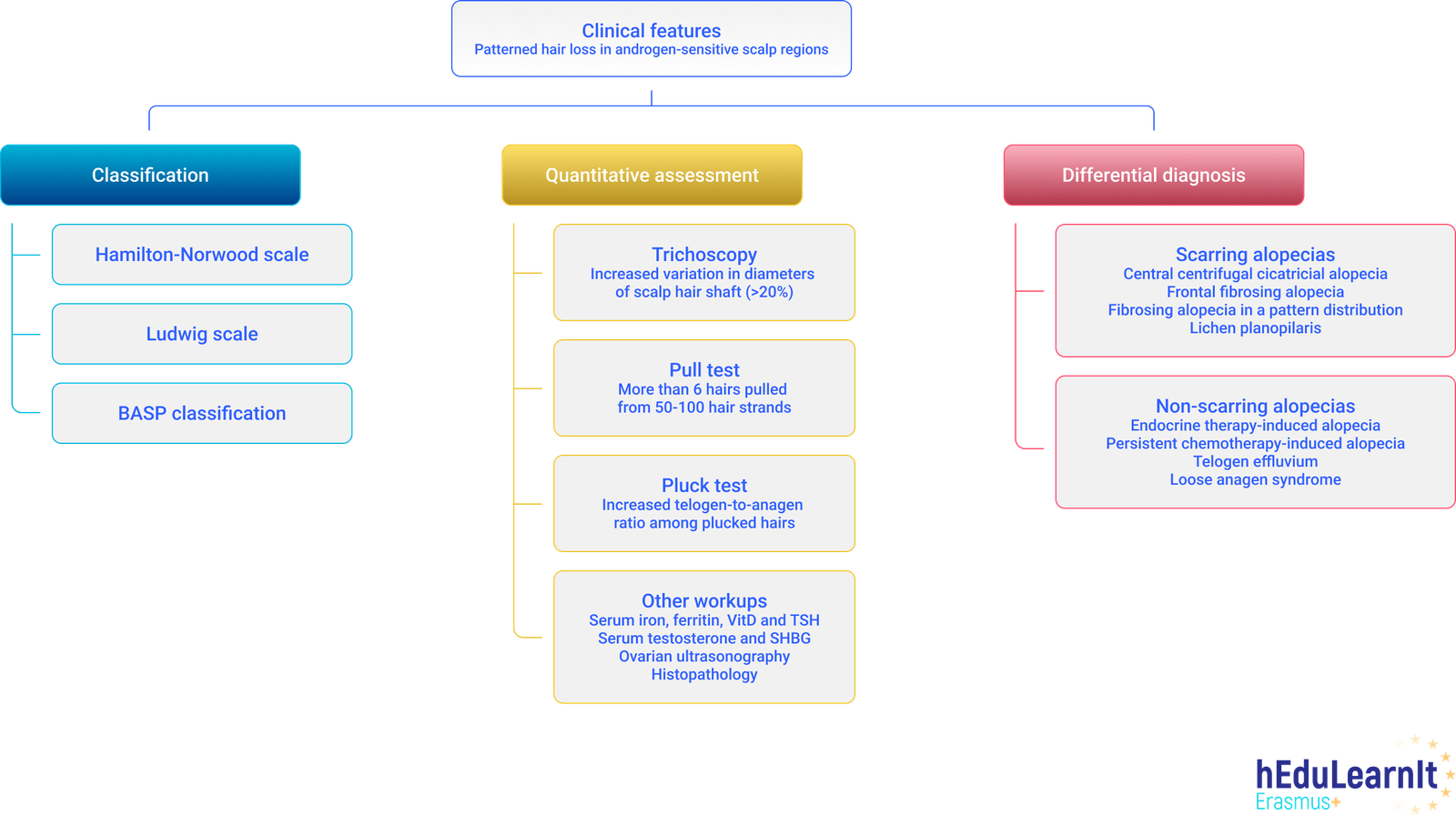
Classification
Female pattern androgenetic alopecia: Ludwig scale I-III.
Male pattern androgenetic alopecia: Hamilton-Norwood scale (typical pattern; anterior pattern or vertex pattern) I-VII.
Laboratory & other workups
Usually not required. Consider endocrinologic evaluation in women with other signs of androgen excess (irregular menses, hirsutism, virilisation). Consider testing for concomitant causes of hair loss (e.g. low ferritin, thyroid dysfunction, lupus erythematosus etc).
Read more
Tests are not usually required. However, an endocrinologic evaluation in women with other signs of androgen excess (irregular menses, hirsutism, virilisation) should be considered. Consider testing for concomitant causes of hair loss (e.g. strict diet with nutritional deficiencies, low ferritin or biotin, thyroid dysfunction, lupus erythematosus).
Dermatopathology
Usually not required. Miniaturisation of the hair follicle with pseudohypertrophy of the associated sebaceous glands, increase in telogen hair follicles.
Read more
A biopsy is only required in cases of diagnostic difficulty (or if multiple causes of hair loss are suspected). Typical histologic findings are of miniaturisation of the hair follicle with pseudohypertrophy of the associated sebaceous glands and an increase in telogen hair follicles. Microscarring in longstanding courses.
Course
Progressive but with highly variable course.
Read more
The course is generally progressive but with highly variable course, in terms of rate of hair loss and distribution.
Complications
Chronic UV damage to the exposed scalp. Long-standing androgenetic alopecia can lead to micro-scarring. Psychosocial problems.
Read more
Loss of hair may lead to chronic UV damage of the exposed scalp and easier trauma. Long-standing hair loss can cause micro-scarring. Sometimes hair loss can lead to psychosocial problems in both women and men. A couple of comorbidities are reported incl. hyperandrogenemia, polycystic ovary syndrome, hypothyroidism, prostate cancer, androgen-secreting tumors, hirsutism, SAPHO or metabolic syndrome.
Diagnosis
Typical clinical findings. Consider a hair pull test and scalp dermoscopy. In women with early androgenetic alopecia, a trichogram (or automated videotrichogram) may be helpful. Excessive androgen production in women must be excluded by history and clinical findings; if other clues of androgen excess are present, endocrine evaluation needed.
Read more
The diagnosis is almost always made on clinical grounds by the typical findings. Consider a hair pull test and scalp dermoscopy in cases of diagnostic difficulty. In women with early androgenetic alopecia, a trichogram may be helpful. Excessive androgen production in women must be excluded by history and clinical findings; if other clues of androgen excess are present, endocrine evaluation is needed.
Differential Diagnosis
Other causes of hair loss e.g. diffuse alopecia areata or especially telogen effluvium in women, long-standing malnutrition with trace elements and vitamins.
Read more
Other causes of hair loss e.g. diffuse alopecia areata or especially telogen effluvium in women. Diffuse hair loss with metabolic deficiencies. Frontal hair fibrosing alopecia. Traction alopecia.
Prevention & Therapy
Minoxidil 2 and 5% solutions, oral finasteride (strict avoidance of pregnancy in women of child-bearing years as finasteride is teratogenic), hair transplantation. Also oral contraceptives with anti-androgens in women. Consider wigs.
Read more
First line topical treatments are Minoxidil 2% and 5% solutions. Systemic administration of Finasteride and oral minoxidil may prevent further hair follicle rarefication (strict avoidance of pregnancy is required in women of child- bearing years as finasteride is teratogenic). Also, spironolactone, oral contraceptives or cyproterone acetate, drospirenone or finasteride are to be considered in women. Hair transplantation may be suitable in some cases. Emerging therapies for AGA include hair follicle-activating peptides, mRNA-containing liposomes, as well as bioengineering of new hair follicles. Psychosocial support and provision of wigs can be considered, especially those with psychosocial issues as a result of the hair loss.
Diagnostic algorithm
Podcasts
References
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment