 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
4.1.4 Hidradenitis Suppurativa
ICD-11
ED92.0
Synonyms
Acne inversa; pyodermia fistulans sinifica.
Read more
Acne inversa; inverse acne; suppurative hidradenitis; pyodermia fistulans sinifica; hidrosadenitis suppurativa; Verneuil disease.
Epidemiology
Prevalence 0.04% (range 0.03%-1%), annual age- and sex-adjusted incidence 6.0 per 100,000. Male:female ratio 1:1.2 to 1:3.3.
Read more
Prevalence 0.04% (range 0.03-1%), annual age- and sex-adjusted incidence 6.0 per 100,000. Increasing incidence over the past four decades particularly among women. Male: female ratio 1:1.2 to 1:3.3.
Definition
Chronic, inflammatory, recurrent, debilitating skin disease (of the terminal hair follicle) usually presenting after puberty with painful, deep-seated, inflamed lesions in the apocrine gland-bearing areas of the body, most commonly the axillary, inguinal, and ano-genital regions.
Aetiology & Pathogenesis
The exact pathogenetic mechanism of hidradenitis suppurativa remains unclear. Smoking, obesity and metabolic syndrome are major predisposing factors.
Read more
The exact pathogenetic mechanism of hidradenitis suppurativa remains unclear. Potential causes are related to genetic, environmental, endocrine and microbiological factors. Follicular keratinocyte differentiation, adipocyte function and inflammation seem to be the major molecular pathogenetic pathways. Sporadic disease 70%, familial disease 30% (mutations at the nicastrin domain within the γ-secretase complex, chromosome 19p13). Smoking (12.6x), obesity (1.1x with every BMI unit; 18% from BMI>30) and metabolic syndrome (4.5x) are major predisposing factors.
Signs & Symptoms
Chronic recurrent inflammatory nodules, abscesses, draining tunnels (sinuses, fistulae and double comedones) and scars.
Localisation
Mostly intertriginous occurrence.
Read more
Mostly intertriginous occurrence in decreasing order of frequency: inguinal, axillary, perineal and perianal, submammary and/or intermammary fold in women, buttocks, mons pubis, scalp, retroauricular area and eyelids.
Classification
Combination of anatomical classification: Hurley I, II, III and severity classification: mild, moderate, severe.
Syndromic hidradenitis suppurativa diseases.
Read more
Combination of anatomical classification (Hurley I, II, III) and severity classification (mild, moderate, severe; IHS4 score). IHS4 can also evaluate HS severity in a dynamic manner.
IHS4 (Points) =
number of nodules x 3 +
number of abscesses x 2 +
number of draining tunnels x4
Mild HS ≤ 3 points
Moderate HS 4 - 10 points
Severe HS ≥ 11 points
Syndromic hidradenitis suppurativa diseases (follicular occlusion, Bazex-Dupré-Christol, Down’s, KID, PAPASH, PASS, PASH, and SAPHO syndromes, Dowling-Degos disease).
Laboratory & other workups
C-reactive protein, erythrocyte sedimentation rate.
Dermatopathology
Heterogeneous histological pattern with hyperplasia of hair follicular epithelium and subepidermal and deep cellular inflammatory infiltrate.
Read more
Heterogeneous histological pattern with hyperplasia of hair follicular epithelium, hyperkeratosis of the terminal follicles, pronounced perifolliculitis, follicle rupture, epidermal psoriasiform hyperplasia, subepidermal and deep cellular inflammatory infiltrate, pronounced acute/chronic dermal inflammation, involvement of apocrine glands and involvement of the subcutis (fat tissue).
Course
Acute and chronic.
Read more
Acute: Recurrent, painful, deep-seated, inflamed nodules with burning, itching, local warmth, and hyperhidrosis.
Chronic: Multiple abscesses, double pseudocomedones, tunels, foul-smelling discharge, scarring, ulceration.
Complications
Squamous cell carcinoma in chronic ano-genital lesions, deep scars, depression, unemployment, change of profession.
Diagnosis
Outbreak of boils during the last 6 months with a minimum of 2 boils in one of the following 6 locations: axilla, groin, genitals, buttocks, under the breasts and perianal area, neck and abdomen regions.
Differential Diagnosis
Staphylococcal infection (furuncle, carbuncle), cutaneous Crohn’s disease , primary or metastatic tumors, lymphogranuloma venereum, apocrine abscess.
Read more
Staphylococcal infection (furuncle, carbuncle), cutaneous Crohn’s disease, primary or metastatic tumors, lymphogranuloma venereum, apocrine abscess, rare diseases (cutaneous actinomycosis, tuberculosis cutis colliquativa).
Prevention & Therapy
Active inflammatory stage
Mild: Topical clindamycin, topical antimicrobials.
Moderate: Oral clindamycin plus rifampicin; tetracycline; adalimumab; acitretin.
Severe: Adalimumab +/- clindamycin/doxycycline.
Chronic including inactive (non-inflammatory) stage.
Local or wide excision.
Prevention
Weight loss and tobacco abstinence, pain management, treatment of secondary infections.
Read more
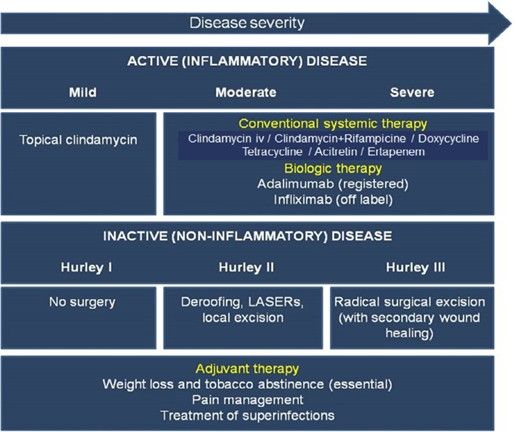
Prevention: Weight loss and tobacco abstinence, pain management, treatment of superinfections.
Special
Comorbid disorders: Inflammatory bowel disease, spondylarthropathy, increased cardiovascular risk.
Syndromic hidradenitis suppurativa diseases are rare.
Differential Diagnosis
Podcasts
Tests
- Peripheral circulatory disturbances with signs such as acrocyanosis and cutis marmorata are possible signs of a predisposition for:
- True or false?
- Which statements apply to hidradenitis suppurativa?
- Statement 1 Hidradenitis suppurativa can on rare occasion lead to bladder or rectal fistulas
- Statement 1 Deodorants are a proven trigger for hidradenitis suppurativa
- What are typical locations for hidradenitis suppurativa?
- Which of the following statements about hidradenitis suppurativa are true?
- Which of the following statements apply to hidradenitis suppurativa?
- Which of the following statements about hidradenitis suppurativa are true?
Further images / DOIA
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment