 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
1.1.1.2 Angioedema
ICD-11
idiopathic: EB04
Read more
Idiopathic: 4A00.15; hereditary 4A0014; drug induced EH61.1; others 4A06.1Y
Synonyms
Quincke edema, angioneurotic / heriditary edema.
Epidemiology
Frequent, but no statistical data available for spontaneous angioedema; prevalence heriditary angioedema 1:50.000 for types I and II, type III rare, females more commonly.
Read more
Angioedema is common. However statistical data depend on the subtype. No exact statistical data are available for spontaneous angioedema, which may be allergic or so called pseudoallergic. The prevalence of hereditary angioedemas is about 1:50,000 for type I (85%) and II. Type III is rare, almost always females are affected. The estimated risk of death caused by asphyxia in patients with HAE is about 8.5 % .
Definition
Acute or slowly progressing dermal and subdermal persistent swellings over several hours to days involving subcutis, mucosa and submucosal tissue. It may occur either as a solitary finding localized or disseminated and following or in parallel with urticaria.
Aetiology & Pathogenesis
Most of the pathogenic causes are histamine related allergic or pseudoallergic following the course of different types of urticaria. Additionally, there are forms without urticaria such as bradykinin-related HAE type I and II (INH-activity partial deficient), III (INH-activity normal). C1-esterase inhibitor deficiency type I and II: renin-angiotensin system related drugs (ACE and dipeptidylpeptidase inhibitors) or paraneoplastic causes.
Read more
Most of the pathogenic causes of angioedemas are of histamine-related allergic or ‘pseudoallergic’ nature, following the course of different types of urticaria. Hereditary forms HAE type I (INH-activity loss) and II (INH-activity partial deficient) are observed where there is no primary urticaria. Type I has an autosomal dominant mutation of the serine protease inhibitor gene 1 (SERPING1). Subtype III has a normal INH-activity and is bradykinin driven. The new Definition, Acronyms, Nomenclature and Classification of Angioedema (DANCE) categorization distinguishes between C1-esterase inhibitor deficiency type I bradykinin-mediated (AE-BK) and type II vascular-endothelial dysfunction-mediated (AE-VE) variants. It often is induced by renin-angiotensin system-related drugs (ACE and dipeptidylpeptidase inhibitors). It may also be a paraneoplastic phenomenon. The gene defect is localized on chromosome 11 subregion q11.2– q13. Kallikrein and factor XIIa cannot be controlled in the acute attack and the bradykinin cascade is activated.
Signs & Symptoms
Subcutaneous and mucosal oedema (upper and lower airways, esophageal-gastro-intestinal tract) with the sensation of tightness or swelling, sometimes itchy or painful.
Read more
Subcutaneous and mucosal oedema (face, upper and lower airways, esophageal-gastro-intestinal and genital tract) with the sensation of tightness or swelling are the main symptoms. Sometimes it can be itchy or even painful. The velocity of lesion development varies from acute to slowly progressing
Localisation
Sites of predilection: face (eyelids, lips), mucosal: tongue, larynx, genitalia.
Classification
Spontaneous and urticaria-related; acquired bradykinin driven without C1-INH deficiency; type I-II hereditary C1 –INH deficiency and type III bradykinin driven without C1-INH deficiency.
Laboratory & other workups
See urticaria for diagnostics. Allergic: IgE, specific IgE, histamine, diaminooxidase. In addition: C1-esterase inhibitor analysis and complement C4 (both concentration + activity). C1-INH and C1q autoantibodies.
Read more
See urticaria for diagnostics. Allergic: IgE, specific IgE, histamine, diaminooxidase, tryptase.
In addition: C1-esterase inhibitor analysis and complement C4 (both concentration + activity). C1-INH autoantibodies and C1q.
Dermatopathology
Edema of the dermal, subcutaneous, submucosal and mucosal tissue without inflammatory infiltrate. Mast cell degranulation.
Read more
Edema of the dermal, subcutaneous and submucosal and mucosal tissue without inflammatory infiltrate. Mast cell degranulation. In drug induced urticaria and angioedema eosinophils are sometimes seen.
Course
Acute onset or progressive development. In allergic and hereditary types chronic relapsing course.
Complications
Airway obstruction, laryngeal oedema, birth delivery complications (be aware of hereditary C1-esterase inhibitor deficiency).
Diagnosis
Clinical, laboratory.
Differential Diagnosis
Physical urticaria (pressure, vibration), autoimmune diseases (e.g. lupus erythematosus), lymphedema, acute phase of herpes zoster and erysipelas. Acute contact dermatitis.
Read more
Depending on acute or slowly developing course. Physical urticaria (pressure, vibration), autoimmune diseases (Lupus erythematosus, dermatomyositis), acute lymphedema, acute phase of herpes zoster and erysipelas, trichinosis. Acute contact dermatitis. Melkersson-Rosenthal syndrome,. Traumatic edema in subcutaneous and muscular tissue.
Prevention & Therapy
Acute: depending on localization and acuity: systemic antihistamines; systemic corticosteroids and adrenaline. For C1-esterase inhibitor deficiency: replacement of C1-esterase inhibitor (if not available, fresh frozen plasma); concentrated C1-inhibitor infusion; bradykinin –B2-receptor antagonist infusion (lanadelumab); recombinant C1 inhibitor. (Danazol or tranexamic acid for long-term prophylaxis only).
Read more
Preventive: if origin and type of angioedema development in relapsing courses of already known underlying disease are explored, avoidance of trigger factors (histamine or bradykinin provoking agents) and in for example hereditary courses substitution of disease associated drugs.
Acute: depending on the localization and the acuity one would either give systemic antihistamines orally or by injection, systemic corticosteroids and adrenaline i.m. (autoinjector). Since very recently, a one way nasal spray containing 2 mg adrenalin as an alternative application way is available. Antihistamines and corticosteroids usually do not interrupt attacks of HAE.
For C1-esterase inhibitor deficiency: replacement of C1-esterase inhibitor (if not available, fresh frozen plasma), concentrated C1-inhibitor infusion, Conestat alfa is a recombinant human (rh) C1- Inhibitor, bradykinin - B2 receptor antagonist infusion (icatibant, lanadelumab), recombinant C1 inhibitor. (Danazol or tranexamic acid for long-term prophylaxis only, however, less used currently). An antisense oligonucleotide PKKRx, also known as donidalorsen, which inhibits plasma kallikrein expression at the messenger RNA (mRNA) level will soon be available. Another oral plasmakallekrein inhibitor for acute attacks is Sebelstratat. Garadacimab, a human monoclonal antibody that inhibits activated FXIIa at the early step of the cascade has been recently launched in Europe.
Suspicious drugs as trigger of acute attacks or maintaining symptoms have to be investigated fully and stopped. Before birth delivery prophylactic recombinant C1 inhibitor should be given or stand by procedure.
Special
In hereditary angioedema genetic counselling is recommended for family members. Postnatal investigation of gene defect presence.
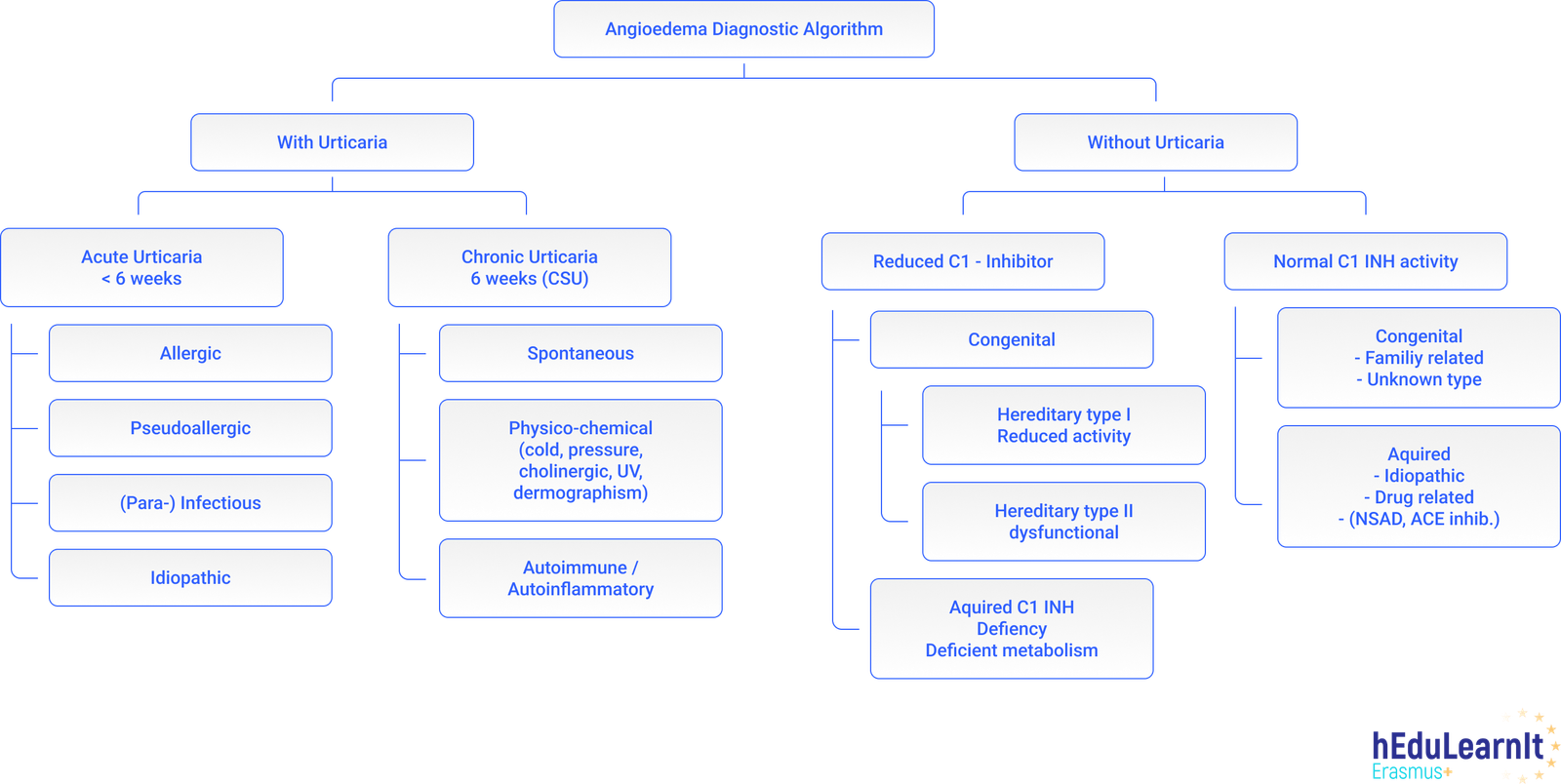
Diagnostic algorithm
Podcasts
Further images / DOIA
Review Articles
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment