 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
10.1.4 Anthrax
ICD-11
1B97
Synonyms
Bacillus anthracis infection.
Epidemiology
Rarely occurring in western countries; endemic in the Middle East, Central Asia and African countries. Annual global incidence is estimated between 2000 and 20,000 cases. Among the three forms (cutaneous, respiratory and gastrointestinal) cutaneous anthrax accounts for 95% of human cases globally.
Definition
Infection with the gram-positive bacteria Bacillus anthracis. Clinical signs depend on the route of infection: inhalation, ingestion, or cutaneous contact.
Aetiology & Pathogenesis
Bacillus anthracis is environmentally stable in spore form and may contaminate soil worldwide, resulting in infections of herbivores. Spores can remain dormant and viable in the environment for decades. Transmission is by inhalation, ingestion, or cutaneous contact with Bacillus anthracis spores in domestic sheep, goat, cattle, wild deer and antelope, through butchering and working with or ingestion of raw or uncooked meat. Incubation period between 1 and 19 days. B. anthracis spores get through the abraded skin into subcutaneous tissues. The toxin produced leads to the characteristic edema and cutaneous ulceration.
Signs & Symptoms
Generally single lesions, sometimes two or more.
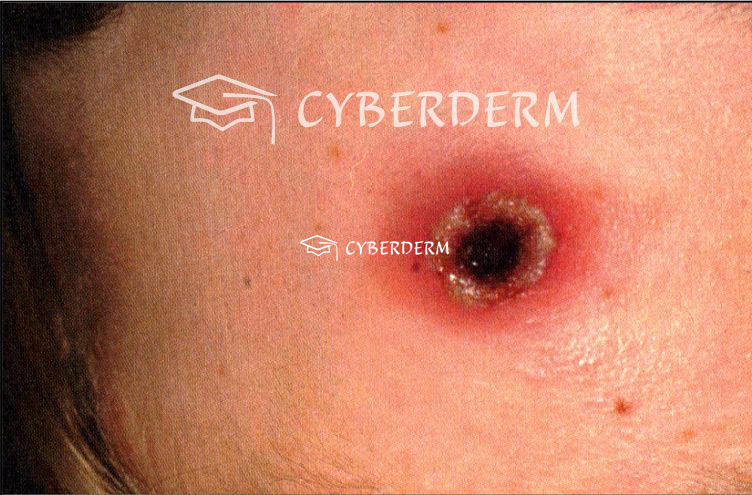
Mild cutaneous anthrax lesion (<4 cm in diameter) centrally depressed vesicle, filled with hemorrhagic fluid and surrounded by a narrow erythema, without systemic symptoms.
Severe cutaneous anthrax: large cutaneous lesion with bullous hemorrhagic reaction, extensive, edema, central (black) necrosis.
Toxemic shock: systemic symptoms (fever, tachycardia and tachypnea).
Localisation
Exposed area of the body, mostly on the face, neck, hands and wrist.
Classification
-
Cutaneous anthrax; clinical course varies from mild to severe.
-
Pulmonary anthrax.
-
Anthrax pneumonia.
-
Pneumonia in anthrax.
Laboratory & other workups
Confirmation is by identification of Bacillus anthracis in a sample, or detection of antibodies or toxins and culturing on sheep blood agar. Peripheral blood count, blood biochemistry and chest X-ray.
Dermatopathology
Hemorrhage, necrosis, and submucosal thrombosis. Staining of the capsule of B. anthracis in the capillaries at the infection site with indian ink.
Course
Hemorrhage, necrosis, and submucosal thrombosis. Staining of the capsule of B. anthracis in the capillaries at the infection site with indian ink.
Complications
Extensive edema, sepsis, toxemic shock and other organ involvement. Healing with scarring in severe cases. Superinfection.
Diagnosis
A detailed history, including the occupation of the patient, exposure to a sick animal or animal products. Demonstration or isolatolation of B. anthracis or gram-positive bacilli from a lesion.
Clinical feature (pustula maligna).
Differential Diagnosis
Staphylococcal skin abscess, cat scratch disease, tularemia, spider bite, and ecthyma gangrenosum.
Prevention & Therapy
Prevention of contact with infected animals or contaminated animal products.
Intramuscular procaine penicillin, oral amoxicillin or penicillin V for mild uncomplicated.
Cutaneous anthrax. Intravenous penicillin G in severe cases. Doxycycline or Ciprofloxacin are alternatives.
Vaccination.
Special
Bacillus anthracis also has been used as a biologic weapon.
Signs & Symptoms

This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment