 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
1.1.4.1 Erythema Nodosum
ICD-11
EB31
Synonyms
Subacute nodular migratory panniculitis.
Epidemiology
2.4/1000 population/year, mostly Spring/Autumn (due to streptococcal infections). F:M = 3-6 : 1. Especially children and adults (20 - 40 years).
Definition
Tissue-reaction pattern with many causes, characterised by painful subcutaneous nodules on the shins, most commonly in women.
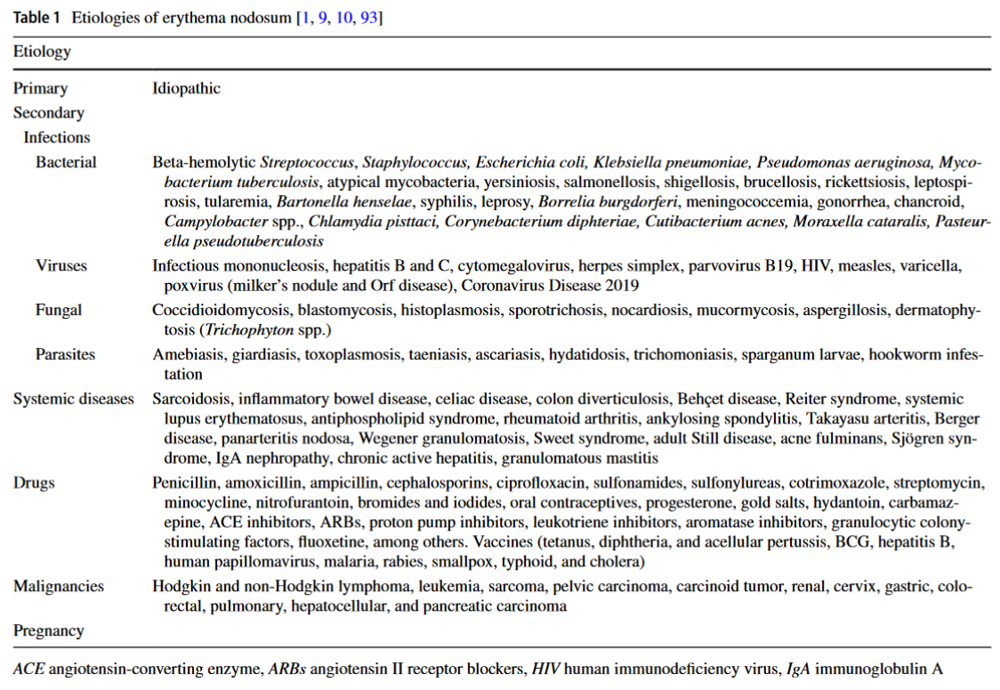
Aetiology & Pathogenesis
Specific common causes include:
- Streptococcal infections
- Hepatitis B
- Sarcoidosis
- Bowel infections (e.g. Yersinia)
- Medications (e.g. penicillins, sulphonamides, oral contraceptives)
- Crohn’s disease
- Tuberculosis
- Other causes such as cat scratch disease and ornithosis.
Pathogenesis
Not well-known. Erythema Nodosum (EN) has been considered a delayed hypersensitivity response to a variety of antigenic stimuli. 30-50% of cases remain idiopathic.
Common causes:
Streptococcal infections
Viral upper respiratory tract infections
Sarcoidosis
Bowel infections (e.g. Yersinia)
Medications (e.g., penicillins, sulphonamides, oral contraceptives)
Crohn’s disease
Tuberculosis
others like, cat scratch disease, ornithosis
Numerous other causes should be considered.
Signs & Symptoms
Often prodrome with malaise, fever, joint pain. Then tender, poorly defined subcutaneous erythematous nodules appear, which are warm to the touch. Over time, colour changes from bright red to dark red to yellow-brownish and finally light grey.
Read more
There is often a prodrome with malaise, fever, joint pain. Then tender, poorly defined subcutaneous erythematous nodules appear (usually bilateral and symmetric), which are warm to the touch. Over time, the colour changes from bright red to dark red to contusiform (bruise-like) to yellow-brownish and finally light grey.
Localisation
Shins (occasionally thighs, buttocks or arms).
Read more
Shins are the most commonly affected area but occasionally the thighs may be affected and rarely buttocks or arms.
Classification
None.
Read more
According to cause.
Laboratory & other workups
Blood tests with several serologic markers (rheumatism, streptococci, tuberculosis, yersiniosis, angioconverting enzyme, pancreatic enzymes, antinuclear antibodies), stool culture and radiographic studies may be considered to exclude some of the known causes. Investigation is dictated by the patient’s history and examination findings.
Dermatopathology
Early phase: inflammatory infiltrate of neutrophils in the subcutaneous fat septae, oedema, macrophages and foam cells.
Later phase: granulomatous reaction and finally fibrous septae with scarring of fat tissue. It is in general a septal panniculitis.
Read more
The timing of any biopsy should be carefully planned (i.e., not too soon after the appearance of the lesions and not too late afterwards). Erythema nodosum is the prototypic of predominantly septal panniculitis. Characteristically, in the early phase, there is an inflammatory infiltrate of neutrophils in the subcutaneous fat septae, edema, macrophages and foam cells. In the later phase granulomatous reaction and finally fibrous septae and scarring of fat tissue occurs. It is in general a septal panniculitis. Miescher’s granulomas can be present. They are highly characteristic, if not pathognomonic and consist and small collections of macrophages surrounding cleft-like spaces.
Course
EN usually heals spontaneously without scarring within 3-6 weeks, however, after longstanding or relapsing lesions, there may be scarring.
Read more
The condition usually heals spontaneously without scarring, however, the eruption may sometimes be longstanding, migrating and/or relapsing. Rarely it may be recurrent depending on the pathogenetic cause. The process usually lasts 3 - 6 weeks.
Complications
Depends on the underlying cause. There are longstanding and migrating subtypes of EN.
Diagnosis
Clinical feature. Occasionally biopsy may be required. A careful search for the underlying disease is needed. Despite investigations, in 25-50% of cases no cause is identified.
Read more
Clinical features are usually diagnostic, but as clinical appearance can be undistinguishable from other panniculitis or even panniculitic-like lymphomas, biopsy is mandatory at least in the first flare of lesions. A careful search for the underlying disease is needed. Despite investigations, in 25-50% of cases no cause is identified.
Differential Diagnosis
Erythema nodosum leprosum; erysipelas; urticaria.
Read more
Polyarteritis nodosa, nodular vasculitis, other forms of panniculitis e.g., trauma, cold.
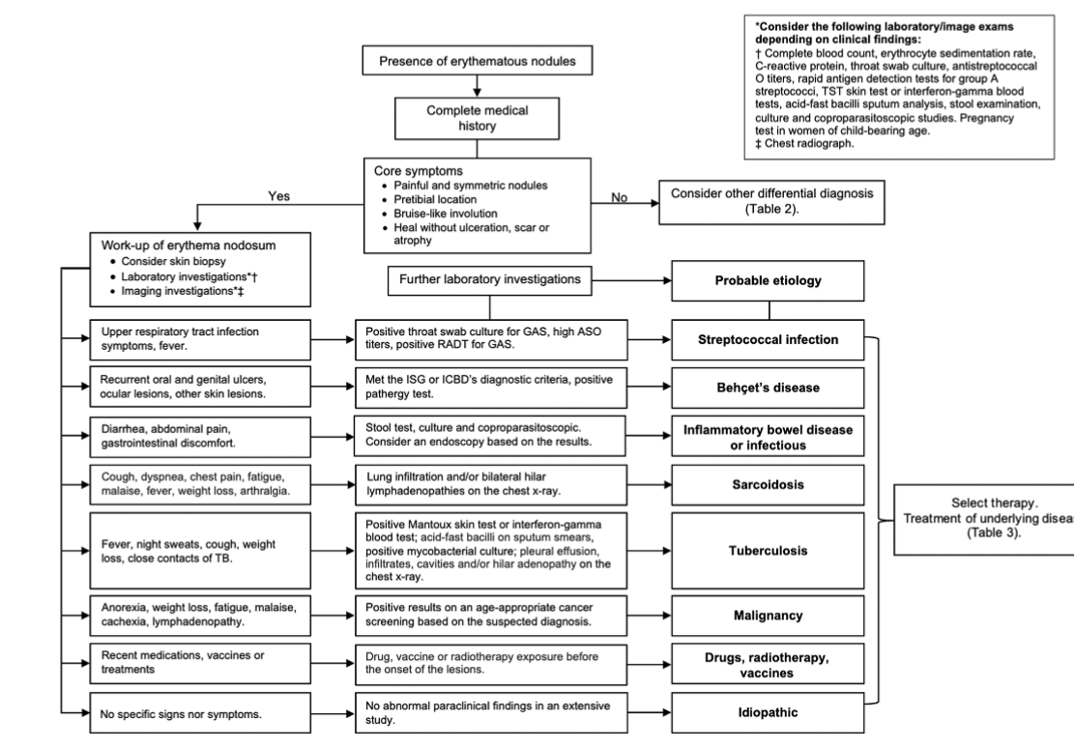
Algorithm for clinical and laboratory approach to check diagnosis of erythema nodosum
Prevention & Therapy
Depends on underlying cause. The underlying disease(s) should be treated. Systemic NSAIDs may be helpful. If the clinical symptoms are severe, short-term systemic corticosteroids may be given. Supportive measures: bed rest, heparinoid creams, and compression stockings.
Read more
Treat underlying disease and consider the administration of systemic NSAIDs. If the clinical manifestations of erythema nodosum are severe, short-term systemic corticosteroids may be given. Potassium iodide is sometimes used for idiopathic and/or recurrent cases. Supportive measures such as bed rest, heparinoid creams and compression stockings may also be helpful.
Special
None.
Podcasts
Further images / DOIA
Review Articles
References
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment