 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
10.5.2 Scabies crustosa (Norwegica)
ICD-11
1G04.1
Synonyms
Crusted scabies; scabies Norwegica; Norwegian scabies.
Epidemiology
Approximately 300 million individuals are affected worldwide each year with scabies. Risk factors for developing crusted scabies include immune deficiency, increased age, dementia, long term immunosuppression, past history of leprosy, special environmental factors (prison), misdiagnosed eczema or prosiasis. Population on risk: aboriginal communities in northern Australia.
Definition
Highly contagious infestation with Sarcoptes scabiei var hominis, mostly seen in immuno compromised patients and showing unhindered proliferation of mites. No special aetiopathogenic or semantic relationship to Norway.
Aetiology & Pathogenesis
Impaired immune status may lead to unlimited spread of mites. Sarcoptes scabiei var. hominis is a human ectoparasite with marked host specificity. Human-to-human transmission occurs with close personal contact, sometimes via clothing or bedding. Female mites (0.3-0.5 mm) dig a burrow in the stratum corneum of the epidermis to lay their eggs; sexually mature mites develop in 3 weeks. Immunologic reaction to mite antigens causes inflammation and pruritus.
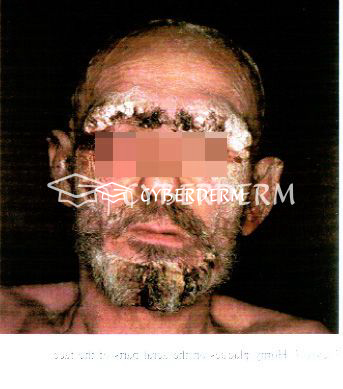
Signs & Symptoms
Erythematous patches develop into thick scaly hyperkeratotic, psoriasiform, fissured, and yellow-to-brown crusted plaques. Unlike classical scabies, pruritus is either mild or absent.
Localisation
Total body. Prediliction sites: fingers, under the nails, and diffusely over palms and soles; elbows and knees.
Classification
A grading scale has been proposed, based on 4 clinical symptoms: the distribution and extent of crusting; the depth of crusting; the degree of skin cracking and pyoderma; and the number of previous episodes.
Laboratory & other workups
Investigation of the immune status. Identification of the mite, its eggs, or scybala (feces) under the dermatoscope or microscope. Blood tests (eosinophilia, anti-nuclear antibodies).
Dermatopathology
Usually not necessary. Acanthosis and hyperkeratosis. Marked thickening of the stratum corneum, containing numerous parasites. Polariscopic examination (birefringence) may be a helpful clue for the visualization of mites and scybala.
Course
Risk of reinfection due to impaired immune status; increased mortality rate.
Complications
Contamination of contact persons and secondary bacterial infection, due to scratching and fissuring of the skin. Septicaemia with increased mortality rate.
Diagnosis
Clinical feature. Identification of mites, eggs or scybala (feces) by dermoscopic, skin scraping or de-roofing burrow with scalpel blade, microscopic examination or reflectance confocal microscopy of burrows.
Prevention & Therapy
Prevention and topical treatment like in conventional scabies.
Systemic treatment: Ivermectin 200 μg/kg (adults and children over 14 kg), together with a fatty meal to improve absorption.
Special
Highly contagious.
Signs & Symptoms

Review Articles
- J.S. Davis, S. McGloughlin, S.Y.C. Tong, et al.: A Novel Clinical Grading Scale to Guide the Management of Crusted Scabies
- V. Palaniappan, H. Gopinath, K. Kaliaperumal: Images in Clinical Tropical Medicine
- L.J. Robertsa, S.E. Huffama, S.F. Walton. et al.: Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment