 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
10.1.1 Buruli Ulcer (BU)
ICD-11
1B21.20
Synonyms
Mycobacterium ulcerans infection.
Epidemiology
West Africa (>70% of global incidence; 50% of cases are children) and some other tropical or subtropical countries. Sporadic imported cases in moderate climate zones.
Definition
Necrotizing and disabling cutaneous disease caused by Mycobacterium ulcerans.
Aetiology & Pathogenesis
Infection with M. ulcerans probably comes from stagnant or slowly moving water; no evidence for human-to-human transmission. Some evidence for mosquitoes as a potential passive vector for M. ulcerans has been reported in some areas. Responsible for the extensive ulceration is an exotoxin called mycolactone, a polyketide-derived macrolide that is synthesized by the M. ulcerans bacteria.
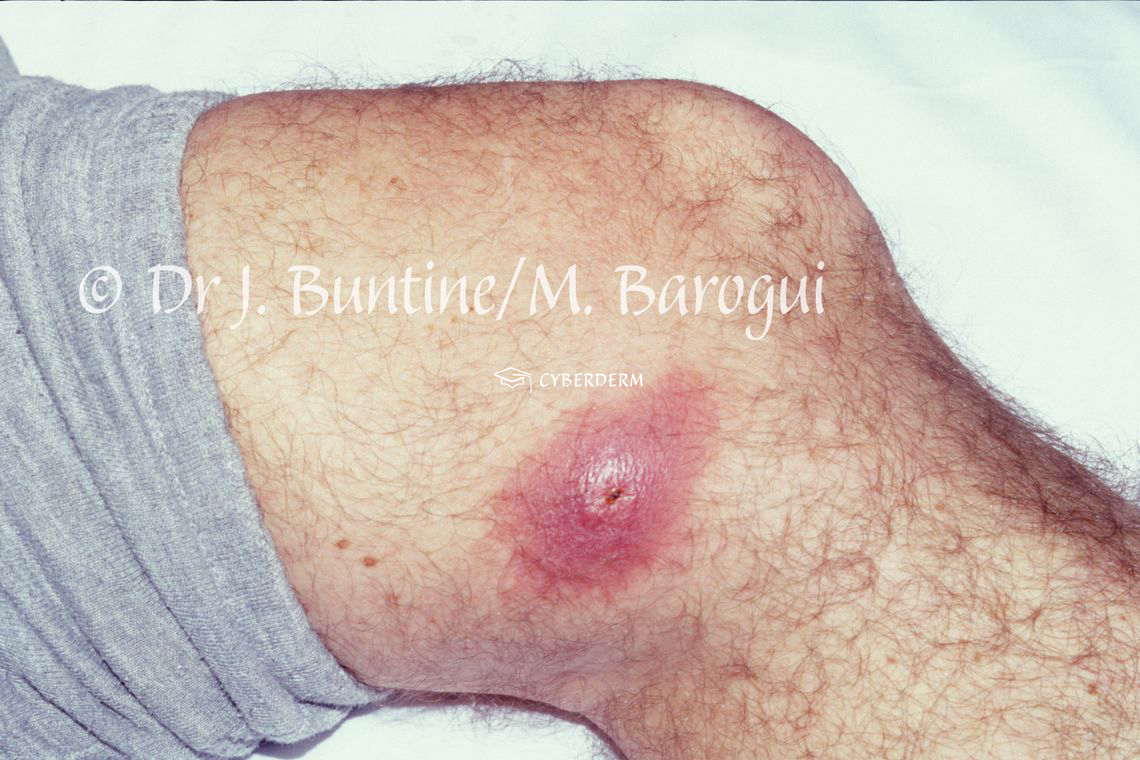
Signs & Symptoms
BU starts with a papule, nodule, plaque, or edematous lesion, progressing to extensive painless ulcer with irregular borders. General health is not affected.
The ulcer grows rapidly with undermined borders. Within 3 weeks to 1 year of evolution, tendons and bone can be involved, leading to osteomyelitis. Most of the time there is a single lesion; however, small satellite lesions can be present.
Depending on the extension, the World Health Organization has classified BU lesions into three categories with some subcategories.
Localisation
Exposed body areas, like limbs or face.
Classification
None.
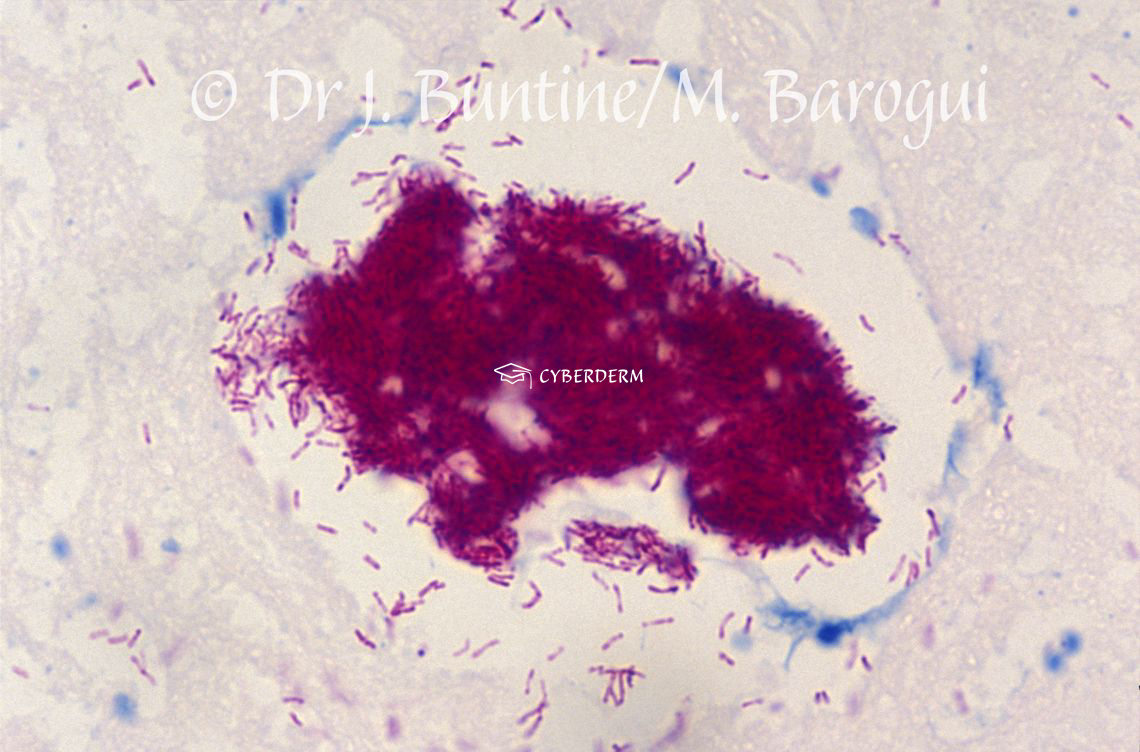
Laboratory & other workups
Acid-fast bacilli in smears or histopathology. Cultering is difficult. Real-time PCR.
Dermatopathology
Hyperplastic epidermis, necrosis, and inflammation. Staining for Acid-fast bacilli.
Course
Chronic leading to disabilities and deformities if not treated. Large scars and contractures leading to functional impairment may further happen due to prolonged ulceration, even under and after adequate treatment.
Complications
Without or delayed antibiotic therapy patients could be left with life-long disabilities and deformities. Paradoxical reaction is the worsening of symptoms during effective antibiotic treatment. Secondary bacterial infections, producing a foul smell.
Diagnosis
Diagnosis relies on clinical, socioeconomic and geographic facts.
Differential Diagnosis
Limb ulcers due to other etiologies.
Prevention & Therapy
Vaccination with Mycobacterium bovis bacillus Calmette-Guérin (BCG) vaccination has been tried, but mostly is uneffective. The best preventative measures are to be careful in risky environments (swimming, fishing) in endemic areas.
Rifampicin (10 mg/kg orally once daily) and streptomycin (15 mg/kg intramuscularly once daily; cave nephrotoxicity and ototoxicity, especially in children) for 8 weeks.
Thorough wound management.
Special
Psychsocial sequelae due to disfiguration.


This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment