 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
1.5.4 Lichen planus
ICD-11
EA91
Synonyms
Lichen ruber planus.
Epidemiology
Prevalence between 0.1 to 4%, with most cases occurring between 30 to 60 years of age, and with a slight predominance in perimenopausal women.
Definition
Idiopathic subacute to chronic inflammatory dermatosis involving the skin, mucosae, nails and/or hair.
Read more
Idiopathic subacute to chronic immune-mediated inflammatory dermatosis involving the skin, mucosae, nails and/or hair.
Aetiology & Pathogenesis
Very likely to be an autoimmune disorder, associations with collagen-vascular diseases, vitiligo and diabetes mellitus. Graft-versus-host-disease (GvHD) has similar morphology. Hepatitis B and C, stress and various drugs may also play a role in its induction.
Read more
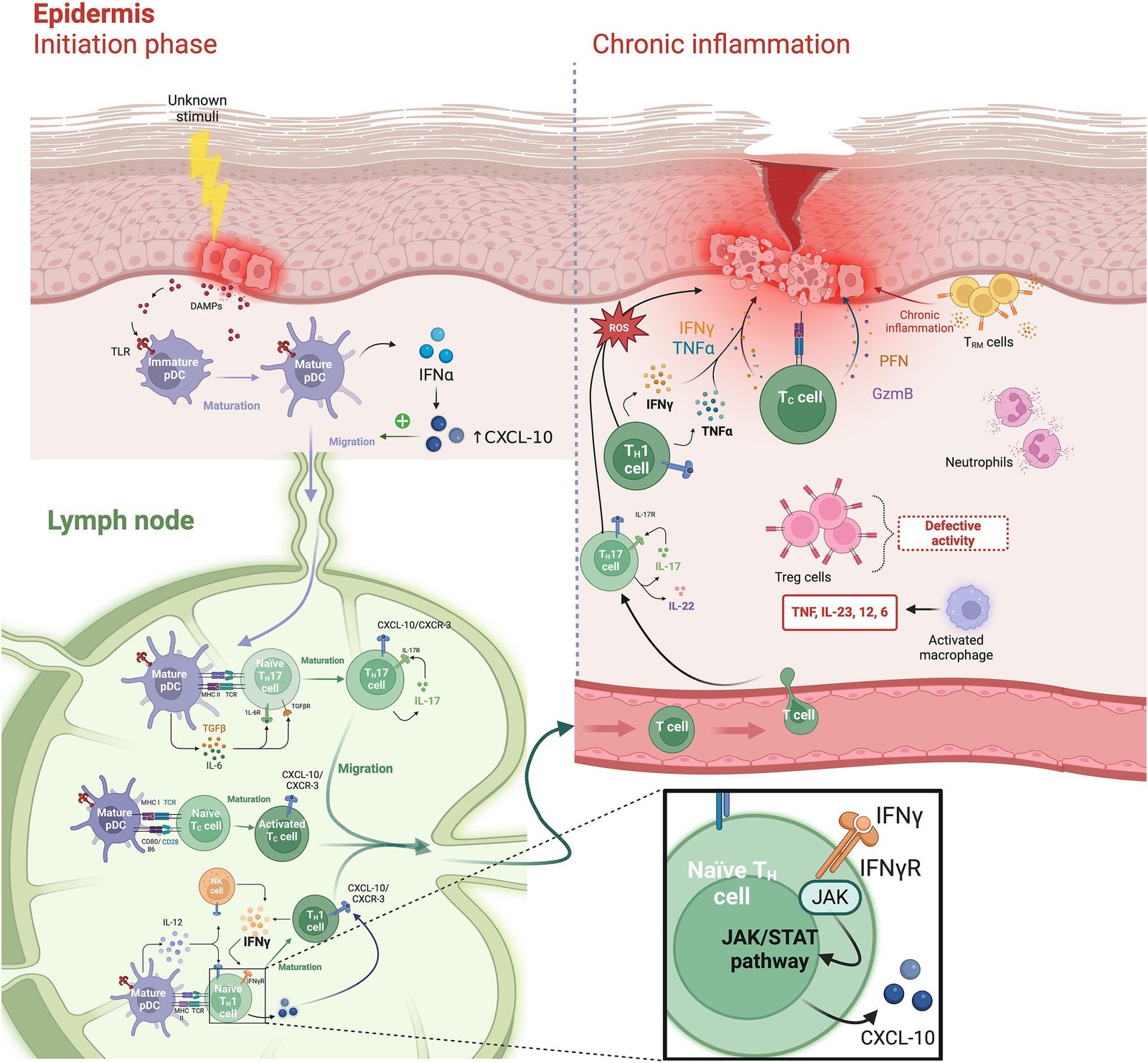
The etiopathology has not been fully elucidated. Very likely it is an autoimmune disorder, thus associations with collagen-vascular diseases, vitiligo and diabetes mellitus are not surprising. Graft-versus-host-disease (GvHD) has similar morphology. An autoimmune biphasic process primarily mediated by CD 4 and CD8 T lymphocytes with cytotoxic mechanisms in response to exogenous or self-altered antigens presented by antigen-presenting cells, such as plasmacytoid dendritic cells (DCs) followed by secretion of type I interferon alpha is currently favoured. Cytotoxic (Th17 and Tc17) lymphocytes by releasing IL–12 and IL–23 are main players. Hepatitis B and C, stress and various drugs may also play a role in its induction in some cases. T-cells accumulate in the upper dermis belonging to the CD4+ and CD8+ subtypes. T-cells, both CD4+ and CD8+, accumulate in the upper dermis. Via secretion of several cytokines apoptosis of basal epidermal cells appear. IFNγ drives the disorder, thus defining LP as a Th1 dominated disorder.
Signs & Symptoms
- Skin: polygonal violaceous papules, white net-like superficial markings (Wickham's striae), marked pruritus; Köbner phenomenon.
- Mucosae: lips, tongue, cheeks, genital and anal areas (annular, bullous, erosive, atrophic), net-like white, non-removable pattern.
- Nails: nonspecific changes (longitudinal stripes), nail dystrophy, nail matrix destruction.
- Scalp: lichen planopilaris, atrophic scarring alopecia.
- Palmoplantar: hyperkeratosis and fissures.
Read more
Five P disease (Pruritic, purple, polygonal, planar papules),
Skin: polygonal violaceous papules, white net-like superficial markings (Wickham’s striae) marked pruritus.
Mucosae: lips, tongue, cheeks, genital and anal areas (annular, bullous, erosive, atrophic), net- like white, non-removable pattern.
Nails: non-specific changes (longitudinal stripes, trachyonychia) but also scarring (pterygium formation, atrophy, anonychyia).
Scalp: lichen planopilaris /lichen planus follicularis decalvans (atrophic scarring alopecia; pseudopelade).
Palmoplantar: hyperkeratosis (fissured).
Localisation
More commonly flexor aspects of wrists, nails, oral and genital mucosae; can be disseminated.
Read more
Flexor aspects of wrists, nails, oral and genital mucosae. Palms and soles.
Classification
Various types: localized, exanthematous, mucosal.
Read more
Types:
Lichen planus exanthematicus -> erythroderma (exfoliative dermatitis),
Hypertrophic lichen planus (lichenification because of chronic rubbing, especially on shins),
Annular or linear lichen planus,
Lichen planus pigmentosus,
Nodular lichen planus,
Atrophic lichen planus (confluent, widespread involvement),
Lichen planus pemphigoides (with antibodies to basement membrane zone),
Erosive lichen planus (bullous, without antibodies),
Actinic lichen planus (hyperpigmentation in sun-exposed sites of individuals of colour).
Laboratory & other workups
None specific.
Read more
Increased Interleukin-6 (IL-6) in serum (not tested on routinary basis).
Dermatopathology
Acanthosis, saw-toothed dermal-epidermal junction profile, hypergranulosis, subepidermal interface band-like infiltrate of T lymphocytes, pigment incontinence.
Course
Lichen planus of the skin often resolves after a few months or years, although it may recur. If caused by medication or tooth fillings, lichen planus will clear after the treatment is stopped or the fillings removed. Lichen planus of the mucosa, nails, and scalp rarely clears by itself and can cause permanent scarring.
Complications
Erosive lichen planus of the mucosae can lead to squamous cell carcinoma, making follow-up essential.
Diagnosis
Clinical features, histology, Köbner phenomenon.
Differential Diagnosis
Lichenoid drug reactions: Skin eruptions caused by commonly used medications can resemble lichen planus. Quinine in tonic water and over-the-counter leg cramp medicines can cause a lichen planus–like condition. In the mouth, allergy to the metals in fillings and oral appliances can cause sores that look exactly like oral lichen planus.
Read more
Lichenoid drug reactions: Skin eruptions caused by commonly used medications can resemble lichen planus. Histopathology shows parakeratosis and eosinophils. Quinine in tonic water and over-the-counter leg cramp medicines can cause a lichen planus–like condition.
In the mouth, allergy to the metals in fillings and oral appliances can cause sores that look exactly like oral lichen planus.
Prevention & Therapy
Prevention: Avoid/control predisposing factors.
- Topical: high potency corticosteroids, calcineurin inhibitors (mucosal involvement), tazarotene, calcipotriol, UVA/B, PUVA, UVA1.
- Systemic: corticosteroids, PUVA, dapsone, hydroxychloroquine, methotrexate, mycophenolate mofetil, acitretin, alitretinoin, ciclosporin, azathioprine, apremilast, sedatives.
Read more
Prevention: Control of predisposing factors.
Topical: high potency corticosteroids, calcineurin inhibitors (mucosal disease; strong evidence), tazarotene, calcipotriol, UVA/B, PUVA, UVA1.
Systemic: corticosteroids (moderate evidence), PUVA, dapsone, hydroxychloroquine, methotraxate, mycophenolate mofetil, acitretin, alitretinoin, ciclosporin, azathioprine, apremilast, sedatives, (enoxaparin, antimycotics).
Special
TNF blockers exhibit fairly controversial effects in lichen planus, since they can trigger proinflammatory reactions.
Read more
TNF blockers exhibit fairly controversial effects in lichen planus, since they can trigger pro-inflammatory reactions: TNF-alpha inhibitors may precipitate lichenoid reactions through disruption of a delicate balance between TNF-alpha and interferon-alpha in susceptible patients. More recent studies focus on Janus kinase inhibitors such as tofacitinib, phosphodiesterase-4 inhibitors such as apremilast, and biologics targeting the interleukin-23/interleukin-17 pathway.
Differential Diagnosis
Podcasts
Tests
- True or false?
- Which diseases are often associated with lichen planus?
- Which therapy is indicated for lichen planus?
- Statement 1 Regular use of sunscreens is an important part of the therapy for lichen planus
- Statement 1 Lichen planus is a dermatologic emergency and must be treated in the hospital
- Which of these diseases does not enter into the differential diagnosis of lichen planus?
- Which of these histological signs suggests lichen planus?
- Which clinical description is typical of lichen planus?
- Which statement regarding lichen planus is false?
Further images / DOIA
Review Articles
- C. Tziotzios, J.Y.W. Lee, T. Brier, et al.: Lichen planus and lichenoid dermatoses: Clinical overview and molecular basis (2018)
- C. Tziotzios, J.Y.W. Lee, T. Brier, et al.: Lichen planus and lichenoid dermatoses: Conventional and emerging therapeutic strategies (2018)
- L. Le Cleach, O. Chosidow: Lichen Planus (2012)
References
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment