 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
10.2.2 Sporotrichosis
ICD-11
1F2J.Z; 1F2J.0; 1F2J.1
Synonyms
Lymphocutaneous and fixed cutaneous sporotrichosis.
Epidemiology
Worldwide distribution. Preferentially in areas with warm, humid, tropical or subtropical climates (Africa, Asia, South America). Young adults is the preferred age group; children are rarely affected.
Definition
Sporotrichosis is a polymorphic subacute or chronic infection by dimorphic fungi of the Sporothrix schenckii complex, which includes several phylogenetically distinct species of dimorphic fungi.
Aetiology & Pathogenesis
Through injury or wounds, inoculation of soil, plants, and decaying material, contaminated with the fungus of the Sporothrix schenckii complex in florists (“Gardner’s disease”). The respiratory route is less common. Transmission also may occur by various animals (rodents). There are various forms of manifestation (see classification). Average incubation time is three weeks. The risk of disseminated disease is increased in immunocompromised patients, or in patients with chronic obstructive pulmonary disease, alcohol abuse, and diabetes.
Signs & Symptoms
Sporotrichosis mostly presents in its cutaneous-lymphatic (>90%) form, with papules, pustules, or linearly distributed, painful or pruriginous ulcerated nodules (chancre), which may develop verrucous plaques in chronic forms and spread along lymphatic vessels.
The second form is cutaneous-fixed sporotrichosis (30% of cases) , which occurs in the same inoculation site (called sporotrichoid chancre), usually consisting of an asymptomatic, sole, vegetative, or slow-growing verrucous lesion, and a squamous, erythematous or violaceous halo
The cutaneous-disseminated (hematogenous ) sporotrichosis is reported in up to 8% of cases and is usually seen in immunocompromised patients. It can manifest at any part of the body surface, and involve even mucous membranes, bones and joints, producing small granulomatous or extensive lytic lesions and osteomyelitis, associated with joint effusions, edema and severe pain.
The extracutaneous forms are less commonly seen, and include disseminated sporotrichosis, pulmonary sporotrichosis and various osteoarticular, ocular and central nervous system disorders.
Localisation
Upper and lower limbs and face.
Classification
Sporotrichosis is classified into cutaneous, pulmonary, and disseminated, with cutaneous being the most common form of the disease (see symptoms).
Laboratory & other workups
Cultures (5 and 8 days; Sabouraud dextrose agar) from exudative lesions, scale, tissue fragment, sputum and blood.
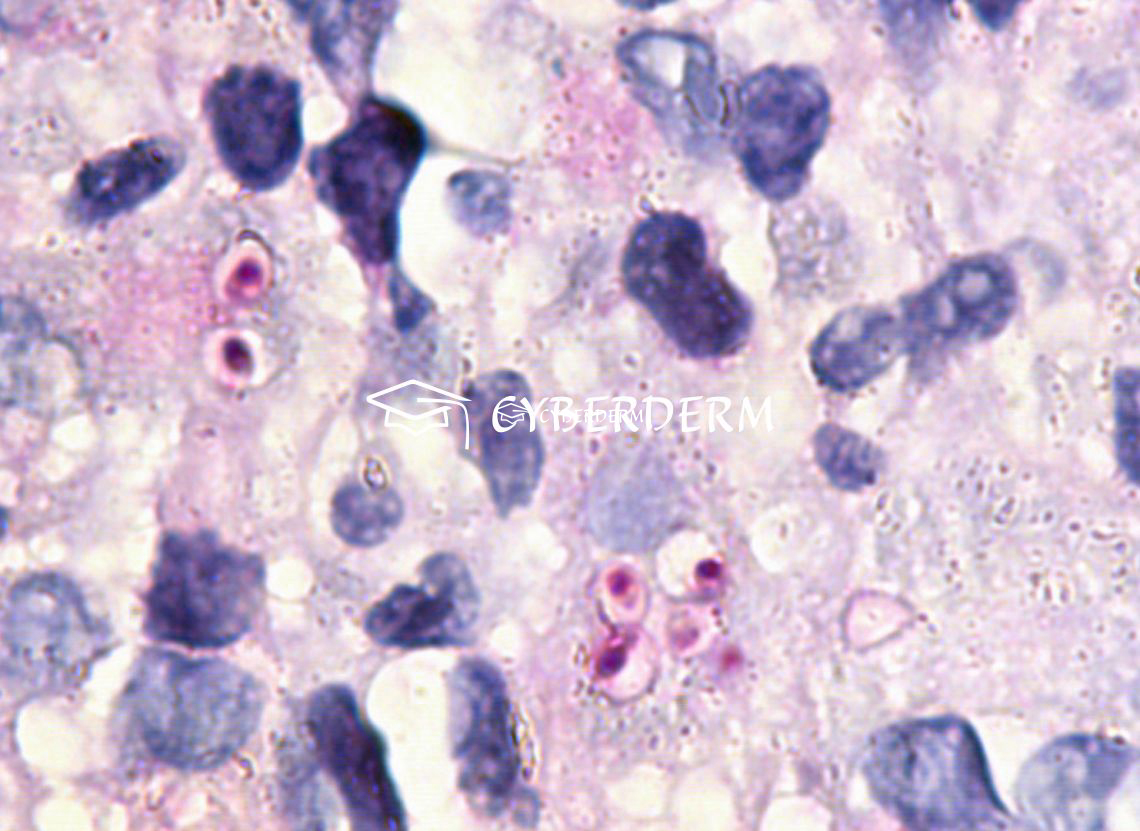
Detection of “cigar-shaped” yeast elements (scarce in cutaneous-lymphatic forms; better to be seen in cutaneous-disseminated or pulmonary, using PAS or Grokott staining). The two main causative agents are Sporothrix schenckii and Sporothrix brasiliensis. Species recognition by Polymerase Chain Reaction.
Dermatopathology
Suppurative granulomas with scarce yeasts and asteroid bodies (PAS and Grocott stains). It must be distinguished from histoplasmosis.
Course
Chronic spread and dissemination.
Complications
Involvement of extracutaneous organs (see symptoms).
Diagnosis
Clinically (“sporotrichoid”) spread along lymphatic vessels.
Differential Diagnosis
Cutaneous Leishmaniasis, histoplasmosis, psoriasis.
Prevention & Therapy
Prevention of trauma.
Cutaneous-lymphatic and cutaneous-fixed sporotrichosis: potassium iodide in diluted solutions.Drug of choice for both clinical forms: itraconazole at 200 mg/day for 3–6 months.
Cutaneous-disseminated, disseminated, pulmonary and osteoarticular sporotrichosis: amphotericin B, 3–5 mg/kg/day.
Special
Cave: confusion with histoplasmosis.
Signs & Symptoms


Review Articles
- R. Morris-Jones: Sporotrichosis
- O. Sizar, R. Talati: Sporotrichosis
- A. Bonifaz, A. Tirado-Sánchez: Cutaneous Disseminated and Extracutaneous Sporotrichosis: Current Status of a Complex Disease
- M. Ramos-e-Silva, C. Vasconcelos, S. Carneiro, et al.: Sporotrichosis
- O. Lupi, S.K. Tyring, M.R. McGinnis: Tropical dermatology: Fungal tropical diseases
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment