 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
10.2.3 Mycetoma
ICD-11
1F29 Eumycetoma.
1C43 Actinomycetoma.
1G60.0 Mycetoma of unknown or unspecified type.
Synonyms
Madura foot.
Epidemiology
The so-called ‘mycetoma belt’ (latitude 15°S and 30°N). It is endemic in Sudan, Somalia, Senegal, India, Yemen, Mexico and Venezuela, and affects preferentially farmers and poor populations in remote areas with higher humidity.
Males are more frequently affected than females (4:1). Age range: 30-40 years.
Definition
Chronic granulomatous infection of the skin and subcutaneous tissue, either by fungi (60%; eumycetoma) or by bacteria (40%; actinomycetoma).
Aetiology & Pathogenesis
-
Causative agents of eumycetoma: Madurella mycetomatis, (most common), Madurella grisea, Pseudoallescheria boydii, Leptosphaeria senegalensis.
-
Causative agents of actinomycetoma: Nocardia spp., including Nocardia brasiliensis, Nocardia asteroids, and Nocardia otidiscaviarum.
Signs & Symptoms
The clinical presentation of eumycetoma and actinomycetoma are almost identical. They involve the skin and subcutaneous tissue, presenting the classic triad of hard woody swelling, painless discharging sinuses and presence of grains (colonies of bacteria or fungi).
Variants:
-
Swelling without sinuses.
-
Cystic type.
-
Verrucous plaque type.
Localisation
Mostly foot, but also any other part of the body.
Classification
See aetiopathology and symptoms.
Laboratory & other workups
KOH
-
Fungal hyphae: periodic-acid–Schiff, Gomori methanamine silver stain.
-
Nocardia species: gram-positive and weakly acid-fast-positive. Actinomadura grains are Gram-positive and acid-fast-negative.
Ultrasound and radiograph, Magnetic resonance imaging (MRI).
PCR and grain cultures.
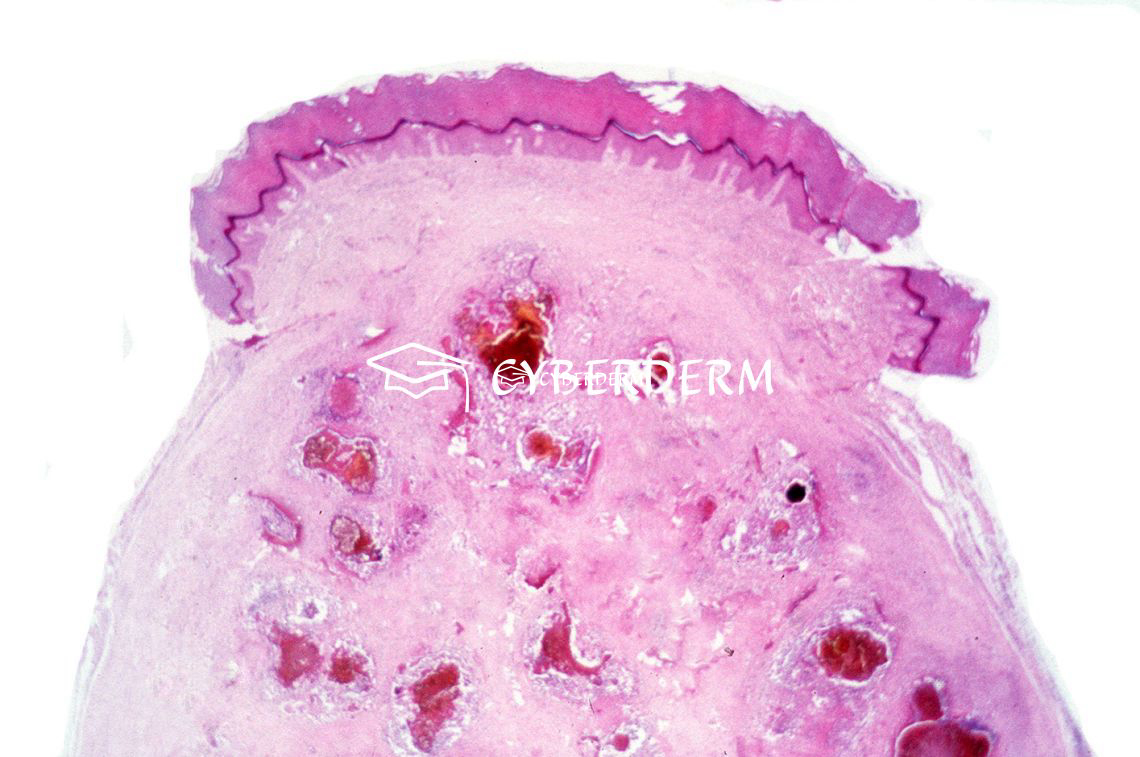
Dermatopathology
Chronic fibrosing inflammation with suppurative granuloma and mycetoma grains. Periodicacid–Schiff (PAS), Gomori methenamine silver (GMS) and gram stains.
Course
Chronic; untreated, the infection spreads through the fasciae and may involve bone and muscle.
Complications
Socioeconomic burden.
Invasion of the periosteum and adjacent bones, leading to osteomyelitis.
Vertebral compression with neurological manifestations when affecting the back.
Rarely lymphatic spread.
Diagnosis
Clinically, histologically, investigation of grains.
Ultrasound and radiograph, Magnetic resonance imaging (MRI) for recognizing the extension of the disease.
Differential Diagnosis
Actinomycosis; aspergillosis; botryomycosis; chromoblstomycosis; coccidioidomycosis; sporotrichosis; tuberculosis; osteomyelitis; neoplasias, podoconisis.
Prevention & Therapy
Surgical treatment is indicated for small, localized lesions and also for large lesions to reduce the organism load. eumycetoma requires a combination of antifungals and surgery and may still have recurrences.
-
Actinomycetoma responds well to antibiotic treatment: Amikacin 15 mg/kg IM divided into two doses + sulfamethoxazole (35 mg/kg/day) and trimethoprim (7 mg/kg/day) divided into three doses for 21 days.
-
Eumycetoma requires a combination of antifungals and surgery and tends to recurre: ketoconazole (400 mg/day), itraconazole (200–400 mg/day), Posaconazole, (200 mg four times daily), voriconazole 400–600 mg/day, amphotericin B (0.5–1.25 mg/kg per day) and terbinafine (500–1000 mg/day), alone or in any combination.
Special
Note: fungal and bacterial mycetoma respectively need completely different therapeutic approaches.
Signs & Symptoms

Review Articles
- O. Lupi, S.K. Tyring, M.R. McGinnis: Tropical dermatology: Fungal tropical diseases
- A.A. Ahmed, W. van de Sande, A. Hassan Fahal: Mycetoma laboratory diagnosis: Review article
- P. Verma, A. Jha: Mycetoma: reviewing a neglected disease
- W.W.J. van de Sande, A.H. Fahal, M. Goodfellow, et al.: Merits and Pitfalls of Currently Used Diagnostic Tools in Mycetoma
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment