 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
8.4 Itching
ICD-11
ME65.1; EC90.6
Synonyms
Pruritus.
Epidemiology
Prevalence: most common symptom in dermatology. Chronic itch 12-20% of general population. In particular, about 60% of the elderly complain of chronic itch. According to different dermatoses or non-dermatoses associated itch, no clear data exists.
Definition
Itching is a symptom of many dermatoses or a symptom of a specific physical or psychological sensation. It produces unpleasant feeling of the skin leading to the desire to scratch.
Aetiology & Pathogenesis
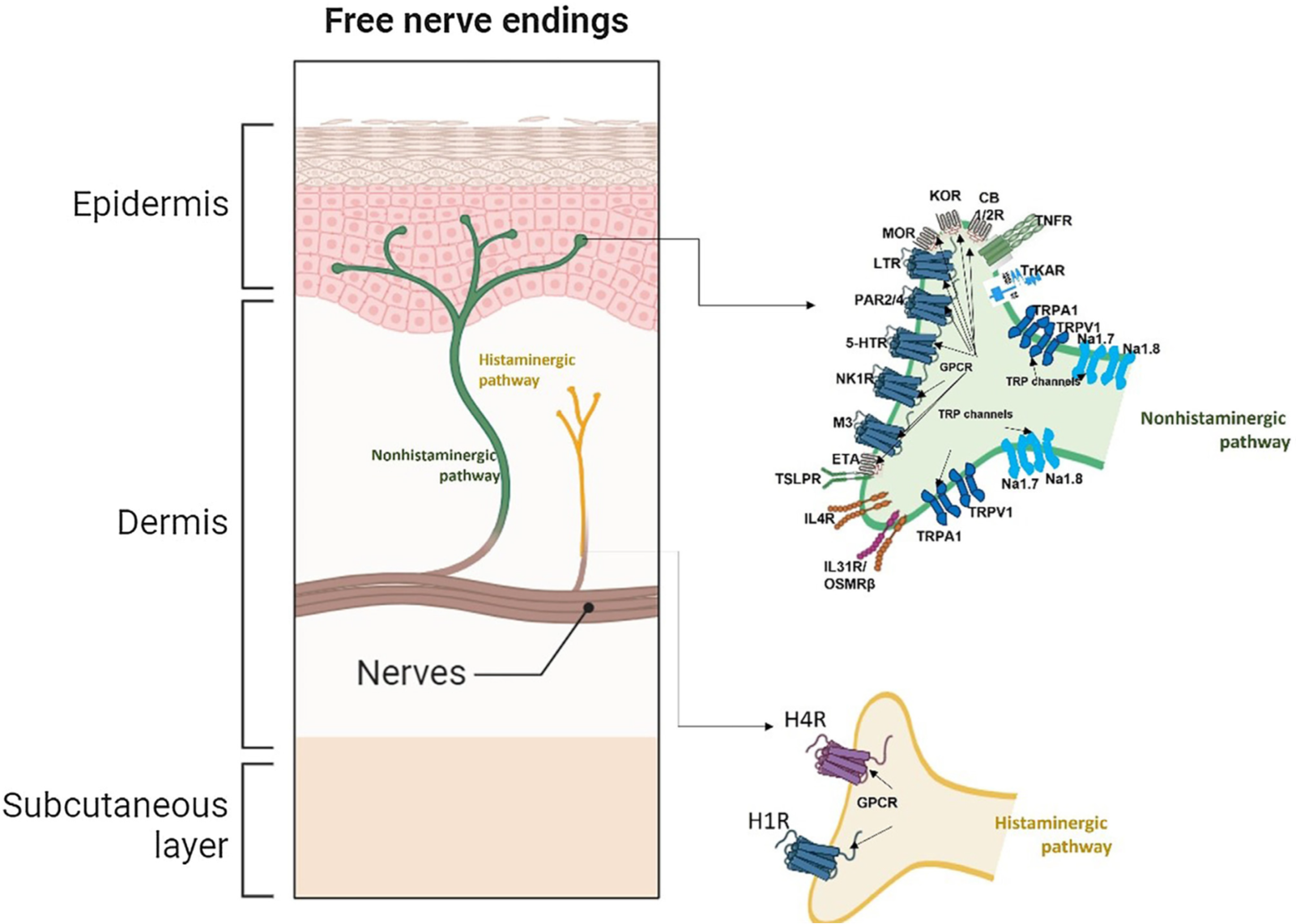
Different stimuli lead to a provocation of scratching in order to remove a pruritogenic factor, a response likely to have originated when most pruritogens were parasites. Dedicated neural pathway (pruritoceptors) similar but different compared to those dedicated to pain, including unmyelinated C fibers and small myelinated Aδ fibers. Itch mediators include histamine, IL-2, TNF-a, IL-4, IL-13, IL-31, thymic stromal lymphoprotein, proteases, neuropeptides (substance P) and opioid peptides.
Read more
Purpose: to provoke scratching in order to remove a pruritogen, a response likely to have originated when most pruritogens were parasites. Dedicated neural pathway (pruritoceptors) similar but different compared to those dedicated to pain, including unmyelinated C fibers and small myelinated Aδ fibers.
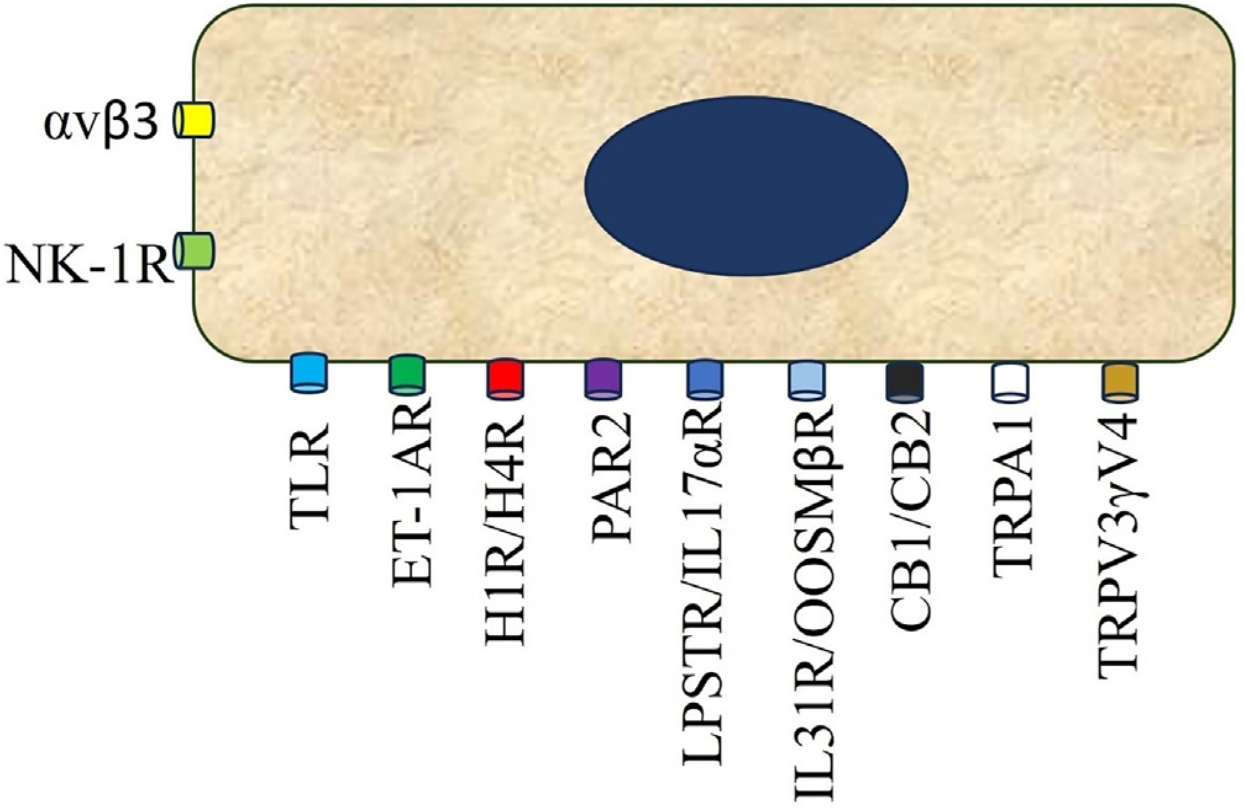
Primary sensory neurons have cell bodies in the dorsal root ganglions and project primary afferents to the skin, and they send projections to the dorsal horn of the spinal cord, where they synapse with second- or third-order neurons, which come together to form part of the spinothalamic tract projecting through the thalamus to the somatosensory and the anterior cingulate cortex. Second- and third-order neurons in the spinal cord may have either excitatory or inhibitory functions. Itch mediators released by resident skin cells and inflammatory cells include histamine, IL-2, TNF-a, IL-4, IL-13, IL-31, thymic stromal lymphoprotein, proteases, neuropeptides (substance P) and opioid peptides.
Signs & Symptoms
Desire to scratch. Quality of itch: burning, painful, stinging, prickling. Itch may be continuous or intermittent (continuous over the day or may come up at certain times during night or may flare up by stress or when patients go to rest).
Localisation
Localized pruritus: usually caused by itchy dermatoses, associated with inflamed skin. Generalized pruritus: can be caused by itchy dermatoses even if the inflamed skin does not show generalized spread, or can be caused by extracutaneous disorders or underlying systemic disorders.
Read more
Localized pruritus: usually caused by itchy dermatoses, associated with inflamed skin, such as in atopic dermatitis, psoriasis, lichen simplex chronicus, tinea, scabies, insect bite reactions.
Generalized pruritus: can be caused by itchy dermatosis even if the inflamed skin does not show generalized spread, or can be caused by extracutaneous disorders.
Classification
- Acute;
- Chronic: Itching lasting 6 or more weeks. Localized or generalized.
- Pruritus with underlying dermatosis (specific skin lesions): atopic dermatitis, eczema, psoriasis, urticaria, scabies, pemphigoid, drug eruptions, cutaneous T cell lymphoma, insect bite reactions.
- Pruritus associated with excoriated nodules and/or lichenification: prurigo nodularis, lichen simplex chronicus.
- Pruritus in patients with normal skin or minimal scratched lesions (pruritus of unknown origin): neurological diseases, hematological disorders, endocrine diseases, infective diseases, uremic, cholestatic, metabolic diseases, neoplastic, drug-induced, psychiatric diseases, mixed.
Read more
Acute or chronic: Itching lasting 6 or more weeks. Localized or generalized.
Pruritus with underlying dermatosis (specific skin lesions): atopic dermatitis, eczema, psoriasis, urticaria, scabies, pemphigoid, drug eruptions, cutaneous T-cell lymphoma, insect bite reactions.
Pruritus associated with excoriated nodules and/or lichenification: prurigo nodularis, lichen simplex chronicus.
Pruritus in patients with normal skin or minimal scratched lesions (pruritus of unknown origin):
Neurologic diseases: multiple sclerosis, brain tumors, small fiber neuropathies, post-herpetic neuralgia, brachioradial pruritus, nostalgia paresthetica.
Hematological disorders: polycythemia vera, myeloproliferative disease, lymphoma.
Endocrine diseases: hyper- and hypothyroidism, hyperparathyroidism, diabetes mellitus.
Infectious diseases: viral hepatitis, parasitoses including helminthosis, HIV/AIDS.
Metabolic diseases: chronic kidney disease, iron deficiency/overload, hepatobiliary diseases and/or cholestasis.
Neoplastic.
Drug induced.
Psychiatric diseases: depression, anxiety, delusion disorders, eating disorders.
Mixed.
Laboratory & other workups
Recommended in patients with pruritus of unknown origin certain blood parameters and imaging techniques as well as biopsy.
Read more
Recommended in patients with pruritus of unknown origin: full blood count, ferritin, urea, electrolytes, liver function test, erythrocyte sedimentation rate (ESR), PCR; chest X-ray. Optional screening test: blood loss investigations, serum bile acids, LDH, beta-2 microglobulin, thyroid function test, fasting glucose HbA1c, calcium, potassium, PTH, vitamin D, HIV, HCV, HAV, HBV, malaria, strongyloidiasis, schistosomiasis; CT scan, magnetic resonance, skin biopsy.
Dermatopathology
It depends on the type of skin lesions present. In chronic itch an increase of nerve fibres in the upper dermis also reaching epidermis can be found.
Course
The course is depending on the underlying disease and may last months or decades. Itch negatively impacts on the quality of life. Severe itch may be devastating.
Complications
Secondary skin lesions caused by scratching. Usually, secondary skin lesions encompass excoriations, ulcerations, crusts, papules, nodules, lichenification, atrophy and scars, hyper- and hypopigmentation. Sleeping disorder. Suicidal ideation.
Diagnosis
In depth case history, physical examination of skin and lymph nodes, assessment of itch severity, screening lab and instrumental tests.
Read more
Accurate anamnesis, physical examination, assessment of itch severity, screening lab and instrumental tests.
Differential Diagnosis
Differentiate pruritus from burning sensations (porphyrias). Specific polyneuropathies.
Read more
Diagnosis of primary skin disorders. Understanding the etiology of pruritus not associated with specific skin lesions.
Prevention & Therapy
Relaxation, mental training, yoga, mindfulness, avoidance of scratching training.
Prevention of dry skin with emollients.
Symptomatic therapy and treatment of underlying disease (where present). Topical treatments: local anaesthetics, topical corticosteroids, topical calcineurin inhibitors. Systemic treatments: antihistamines, short term corticosteroids, ciclosporin. Opioid receptor agonists and antagonists, antiepileptics. Antidepressants, neurokinin antagonists, biologics. Ultraviolet phototherapy.
Read more
Symptomatic therapy and treatment of underlying disease (were present). Topical treatments: local anaesthetics, topical corticosteroids, topical calcineurin inhibitors. Systemic treatments: antihistamines, short term corticosteroids, ciclosporin. Opioid κ receptor agonists (nalfurafine, difelikefalin) and μ receptor antagonists (nalmefene, naltrexone), antiepileptics (gabapentin, pregabalin). Antidepressants (paroxetine, fluvoxamine, sertraline, amitriptiline, mirtazapine), neurokinin antagonists (aprepitant, serlopitant), anti-IL-4/IL-13 antibodies (dupilumab), anti-IL31R (nemolizumab). Ultraviolet phototherapy.
Special
None.
Review Articles
References
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment