 English
English
 German
German
 French
French
 Italian
Italian
 Spanish
Spanish
 Portuguese
Portuguese
 Chinese
Chinese
 Lithuanian
Lithuanian
1.1.3.5 Toxic Epidermal Necrolysis
ICD-11
Synonyms
Lyell syndrome
Epidemiology
Rare disease 1-2 per 1 million. Higher risk in HIV/AIDS.
Read more
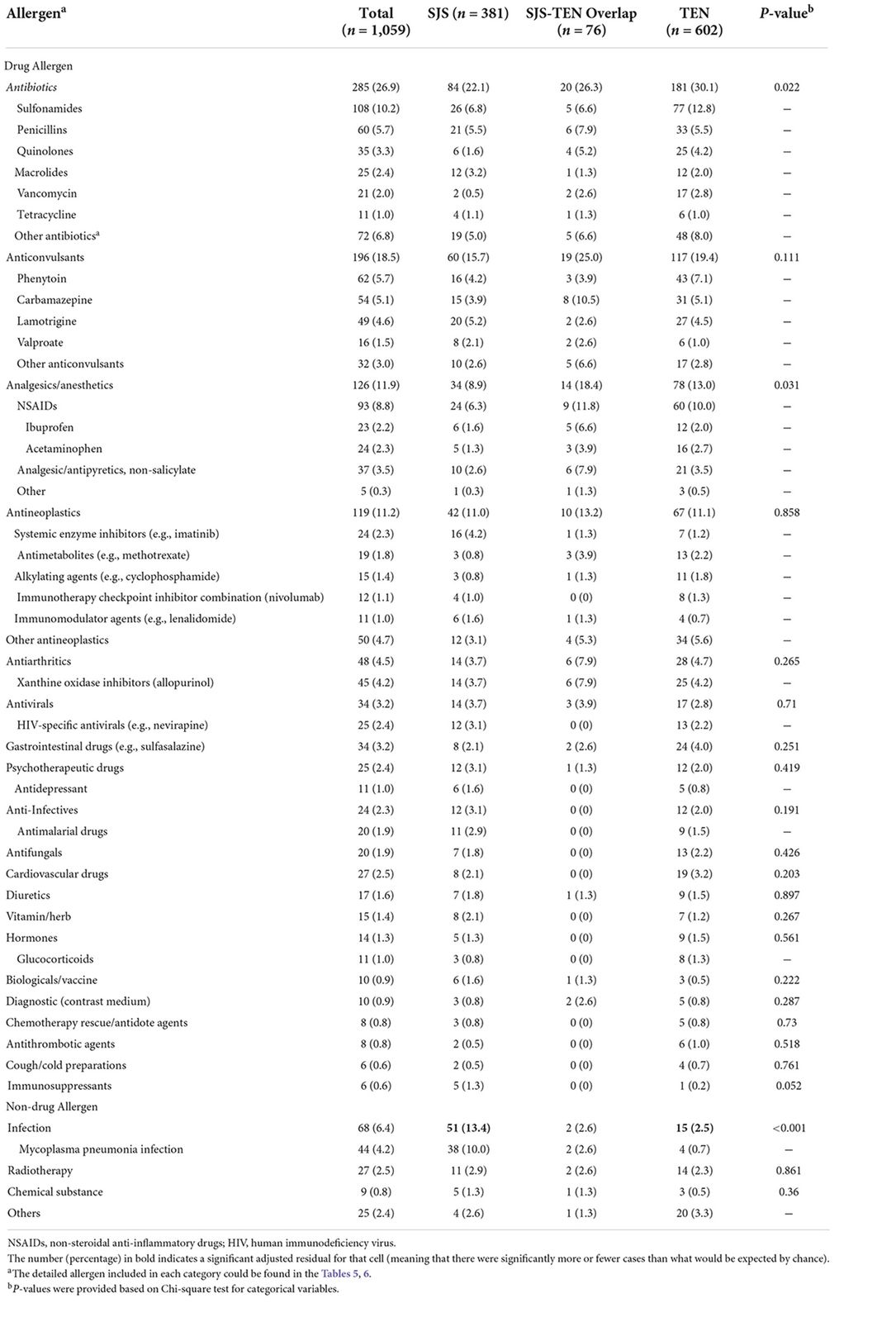
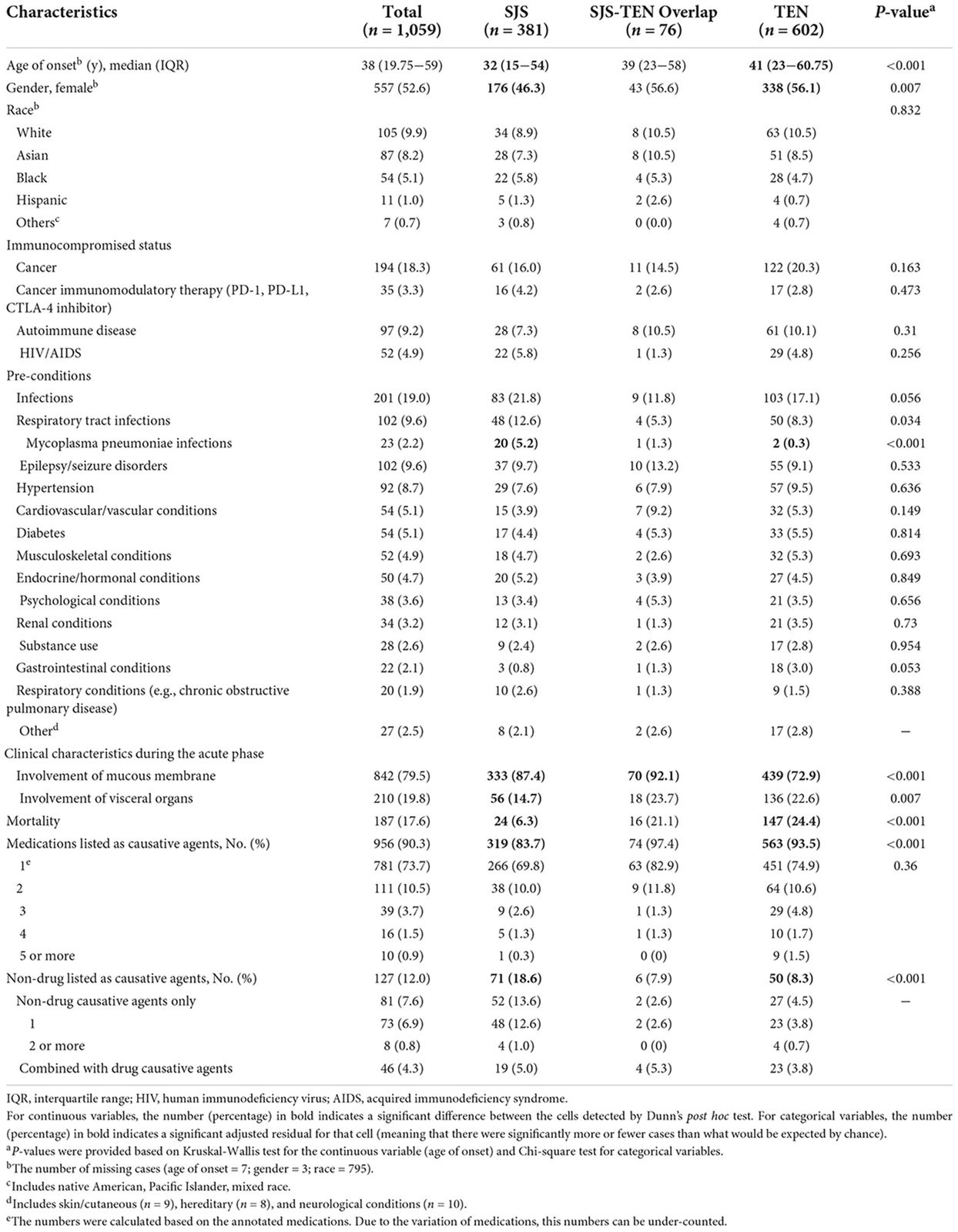
Toxic epidermal necrolysis (TEN) is a rare disease affecting around 1-2 persons per 1 million. There is a higher risk of developing this serious disease in HIV/AIDS patients and in elderly patients receiving multiple medications. 7−10% of cases in all groups have at least one autoimmune disease. There are new data showing that infections is highest among SJS cases (21.8 %) compared to TEN (17.1 %) and SJS_TEN overlap (11.8%).
Definition
Severe drug-induced skin reaction characterised by death of the epidermis (keratinocyte necrosis) and marked mucosal erosions. Part of a spectrum, which ranges from SJS, where 30% of the BS is referred to as SJS-TEN-overlap syndrome.
Read more
Toxic epidermal necrolysis (TEN) is a severe drug-induced skin reaction characterised by death of the epidermis (keratinocyte necrosis) and marked mucosal erosions. It is part of a spectrum of severe drug eruptions, affecting skin and the oro-genital mucous membranes and conjunctivae. The body surface (BS) involvement differs from SJS, where <10% of BS is affected to toxic epidermal necrolysis (TEN) in which 30% of the BS shows loss of the epidermis. Involvement of 10 to 30% of the BS is referred to as SJS-TEN-overlap syndrome.
Aetiology & Pathogenesis
Triggers are medications (typically antibiotics and antiepileptic drugs). Immunologically-induced apoptosis of keratinocytes cascading unchecked into massive epidermal destruction may be the pathogenic mechanism. Necrolysis by TNF alpha and gamma IFN. AnnexinA 1 promotes apotosis of keratinocyes. Increased miR-18 a-5p which is blocking antiapotopic action.
Read more
There are many causes of TEN. Whereas in Erythema exsudativum multiforme (minor and major type) infections such as viruses e.g. the herpes virus and mycoplasma are important aetiological factors, much more often in Stevens-Johnson syndrome and in toxic epidermal necrolysis, drugs are the inducing agents. Immunologically-induced apoptosis of keratinocytes cascading unchecked into massive epidermal destruction may be the pathogenic mechanism. Beside multi-drug exposure in particular in the elderly population, hereditary disposition to severe cutaneous drug reactions is an additional risk. In Chinese and Thai patients SJS/TEN induced by carbamazepine shows a high correlation with HLA-B*1502.This correlation is not found in the European population, but rather an association with HAL class I-allelel HLA-A*3101. In all populations, TEN is often induced by the very common drug allopurinol (minimal daily dose 200 mg). An association with HLA-B*5801 can be detected in that case. Necrolysis by TNF alpha and gamma IFN are important mediators of the cell changes. Annexin A 1 promotes via the formyl-peptid- receptor apoptosis of keratinocytes and an increased level of miR-18 a-5p in the skin can be measured, which blocks antiapoptotic action and therefore promotes cell death. Current theories involve apoptosis due to FAS-mediated mechanisms, granulysin and reactive oxygen species. Recently, the inflammatory JAK/STAT pathway has been detected as the main driver of disease.
Drugs with high risk:
allopurinol,
carbamazepine, lamotrigine, sertraline, phenytoin, nevirapine, phenobarbital,
piroxicam,
sulfamethoxazol, sulfsalazine and other anti-bacterial sulfonamides.
Drugs with moderate risk: cephalosporines, quinolones, macrolides, NSAIDs e.g. diclofenac and tetracyclines
> for further details see tables
Signs & Symptoms
Starting with a confluent maculopapular exanthem without the classical E.e.m. like lesions, haemorrhagic blisters, epidermal necrosis followed by loss of sheets of epidermis; positive Nikolski's signs (Nikolski I: blisters induced by rubbing normal skin. Nikolski II: existing blisters extend with lateral pressure); usually severe periorificial mucosal erosions.
Read more
As in SJS, initially a macular exanthem develops, usually on the trunk. In contrast to erythema exudativum multiforme, the typical target lesions of cockades are not seen. Fever, conjunctivitis, sensitivity to daylight and artificial light and throat pain often precede the skin symptoms.
After skin symptoms have started on the trunk, the face and hands and feet follow, often becoming confluent, with formation of atypical target lesions without the classical E.e.m.-like characteristics. Erosions and even ulcerations may appear. More than 30% of body surface is involved. Erosions generally present around more than one mucosal orifice. Later balanitis may be seen and the upper respiratory and gastrointestinal tract are involved. The Nikolsky I skin sign is positive.
Localisation
Skin and mucosa.
Read more
Skin and mucosa including esophagus are both affected.
Classification
Part of the Erythema multiforme –SJS/TEN complex as the maximal variant of the clinical cascade.
Read more
Toxic epidermal necrolysis is the worst part of the spectrum of the Erythema exsudativum multiforme – SJS -TEN complex which can be seen as a clinical cascade, however, the course of Eem min general is milder.
A prognostic scoring system (SCORETEN) should always be used. Every parameter which is positively answered is ranked with one scoring point:
Age > 40 years /malignant tumor(s) / skin ablation > 10% BSF / heart frequency > 120 pro min / bicarbonate < 20mmol per liter / urea > 10mmol per liter / hyperglycemia > 252 mg/dl.
More than 50% of TEN patients suffer from long-term sequelae.
Laboratory & other workups
Check electrolytes, kidney and liver parameters, cardiac function.
Read more
Regular monitoring of electrolytes, kidney and liver parameters and cardiac function is essential.
Dermatopathology
Cytotoxic CD8 T-lymphocytes attacking the epidermal keratinocytes, but also mucous epithelia. Apoptosis and necrosis of cells. Disruption of epidermal / dermal connection. Bulla formation because of severe epidermal necrosis. Epidermal remnants separated from dermis with only sparse inflammatory infiltrate.
Read more
Cytotoxic T-lymphocytes attack the epidermal keratinocytes, but also mucous epithelia are involved. Apoptosis and necrosis of keratinocytes is the key feature. Disruption of the epidermal/dermal connection leads to formation of large bullae. Capillaries in the upper dermal vessel complex are widened and a heavy lympho-mononuclear cell infiltrate is assembled.
Course
More than 40 % complications. 30% mortality rate. More than 50% of TEN patients suffer from long-term sequelae.
Read more
The course of disease depends on age, comorbidity, body function surface involvement, body functional status and how early treatment is commenced. Intravenous electrolytes and bicarbonate should be balanced and the patients should be monitored analogously to burn patients with a degree IIa and III.
The 30% mortality rate and > 40% complication rate is very high. Typically, sequelae may leave scarring areas of skin and mucosa.
Complications
Infection, electrolyte and fluid disturbances. Ophthalmic involvement incl. ectropium and synechia, phimosis, vaginal synechia. Scarring in esophagus and mouth mucosa.
SCORTEN evaluation essential.
Read more
Long-term sequelae such as scarring of the blepharon, development of an ectropion, phimosis and vaginal synechia are often seen. Scarring in esophagus and mouth mucosa are common. During the acute phase of the disease, electrolyte and fluid disturbances are very common.
Diagnosis
Clinical features and histology, showing necrolysis throughout all epidermal layers.
Read more
The clinical features and the histology show necrolysis throughout all epidermal layers, which confirms the diagnosis. Usually, inflammatory infiltrate in the dermis is mild.
Differential Diagnosis
Staphylococcal scalded skin syndrome, burns, erythema multiforme, Disseminated fixed drug eruption, pemphigus and pemphigoid variants and linear IgA disease.
Read more
Staphylococcal scalded skin syndrome,
generalized subcorneal pustulosis at the early stage,
burns,
disseminated erythema multiforme major type, disseminated fixed drug eruption, DRESS,
pemphigus and pemphigoid variants and linear IgA disease.
Prevention & Therapy
Immediate referral to special dermatologic and intensive care center.
Aggressive burn therapy (fluid and electrolyte management, appropriate antibiotic coverage, warming measures), special supportive.
According to course and BS and mucosal involvement. Intravenous immunoglobulins, TNF alpha blockers. High dose ciclosporine and / or systemic corticosteroids. Ophthalmology review.
Read more
All suspicious drugs have to be discontinued. Drug half-life should be known because it will influence the response rate and time of treatment length to avoid immediate relapse. The systemic use of ciclosporin (3 mg/kg/day) is currently favoured. Alternatively, corticosteroids in a pulse with 0.5 to 1.1 g/d, TNF alpha blockers or intravenous immunoglobulins in high dosages appear helpful if the disease continues to progress even after the triggering medication has been stopped. Although there is some debate in the literature, intravenous immunoglobulin has been shown to be effective when given early in the course of TEN. Symptomatic topical measures are essential to avoid superinfection and scarring similar to burn patients. In 2024 it was published that targeted inhibition with YAK/ STAT inhibitors in vitro reduced keratinocyte-directed cytotoxicity. In vivo oral administration of tofacitinib, baricitinib or the JAK1-specific inhibitors abrocitinib or upadacitinib ameliorated clinical and histological disease severity in two distinct mouse models of TEN. Based on these findings treatment with JAK inhibitors (JAKi) was safe and associated with rapid cutaneous re-epithelialization and recovery in seven patients with TEN.
Early and aggressive interventions like those used for burns patients (fluid and electrolyte management, appropriate antibiotic coverage, warming measures) are standard. Special technical support (e.g., special bed, metalline bandages) are recommended. Patients are ideally treated on an intensive care unit. Regular ophthalmologic monitoring may help to avoid blepharon development.
Special
Ophthalmologic consultations.
Read more
Genetic testing for susceptibility and entry on the European Register is recommended.
Demographics and clinical characteristics of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) cases from PubMed/MEDLINE.
Differential Diagnosis
Podcasts
Review Articles
References
This website uses cookies!
We use cookies to tailor our content to your needs and continuously improve our website. You can decide which cookies you want to allow. Detailed information about the cookies we use can be found in our Privacy Policy and Cookie Settings. You can withdraw your consent at any time.
Comments
Be the first one to leave a comment